23 Nov 2015
Darragh Kelly
Job Title
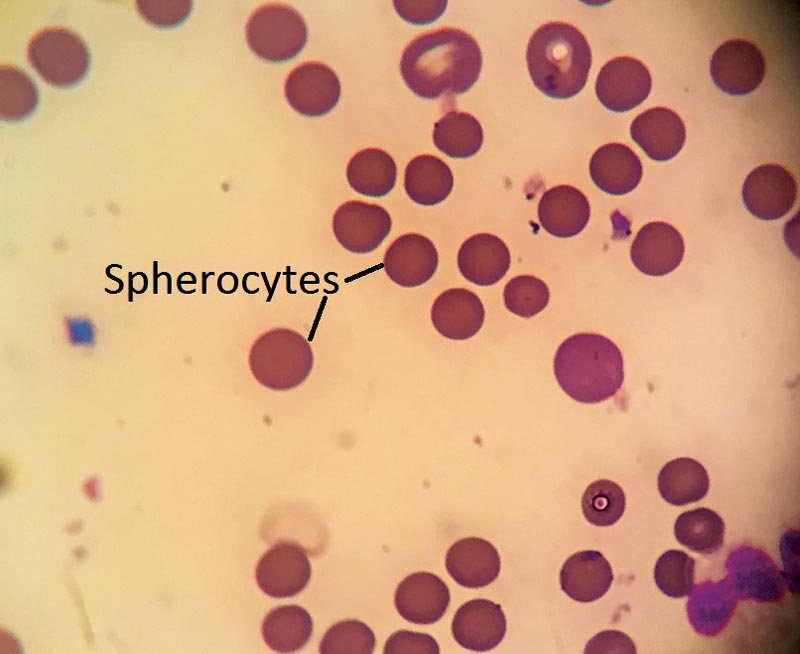
Figure 2. Blood smear with multiple spherocytes.
Tia, a three-year-old female, neutered cocker spaniel, is presented at your practice as an emergency with lethargy and weakness. She is non-ambulatory. The owner reports Tia had passed bloody urine earlier in the day.
Tia has no previous health issues, no travel history, no known access to toxins and is up to date with parasite prophylaxis and vaccinations.

Clinical examination reveals pale, icteric mucous membranes, slight pyrexia, tachycardia and bounding peripheral pulses. A mild splenomegaly is detected on abdominal palpation. In-house haematology reveals a severe anaemia with a PCV of 15%. Hyperbilirubinaemia is evident, but serum biochemistry is otherwise unremarkable.
The plasma was pink (Figure 1), which can be caused by intravascular haemolysis.
The total protein (TP) was normal. A normal TP is more typical in dogs with haemolytic rather than blood loss anaemia.
Multiple spherocytes were seen on the smear (Figure 2). Spherocytes are small, round, intensely stained RBCs that lack central pallor and are created by mononuclear cell phagocytosis of a portion of antibody-coated RBC membrane. Although not pathognomonic, marked spherocytosis is highly suggestive of immune-mediated haemolytic anaemia (IMHA). In Tia’s case a normal number of platelets were seen in the monolayer (10 to 12 per high power field), which makes Evans syndrome (concurrent IMHA and thrombocytopenia) unlikely.
A positive slide agglutination test is common in animals with IMHA. This is carried out by mixing one drop of anticoagulated whole blood with one drop of saline on a glass slide. Agglutination was visualised grossly in Tia’s case (Figure 3).
Tia had pigmenturia and urine sedimentation was performed on a free catch sample (Figure 4). Microscopic examination revealed haemoglobinuria, which can be caused by intravascular haemolysis.
Icterus and splenomegaly are frequently seen in haemolytic anaemias. Primary IMHA is well recognised in cocker spaniels.

On the basis of these in-house tests it was decided Tia had an intravascular haemolytic anaemia with an immune-
mediated component. Further tests should then look for a possible underlying cause of the IMHA.
IMHA can be divided into primary and secondary conditions. Between 60% and 75% of IMHA cases are primary (idiopathic). Secondary causes include neoplasia, focal infections, blood-borne parasites, certain drugs, intrinsic RBC defects and other causes, such as onion and zinc toxicity.
Diagnostic imaging should be performed to look for underlying causes and a blood smear can be sent to the laboratory for evaluation and to check for blood borne parasites (+/- serological testing). A Coombs test, which detects antibodies attached to RBCs, can be carried out in patients with anti-RBC levels that are too low to cause agglutination.
In Tia’s case a diagnosis of primary IMHA was made. Treatment included a blood transfusion and immunosuppressive doses of glucocorticoids. Aspirin was also administered to reduce the risk of disseminated intravascular coagulation and thromboembolic disease.
Tia responded well to therapy, but it must be noted complete response to treatment can take weeks to months and some patients may require lifelong therapy.
In conclusion, by following a series of tests it is possible to classify the anaemia and make a rapid yet confident diagnosis of IMHA in an emergency situation.