29 Oct 2018
Francesco Cian presents a case from a dog with a four-day history of acute history of acute cervical hyperaesthesia and neurological deficits on the frontal limbs.
Francesco Cian
Job Title
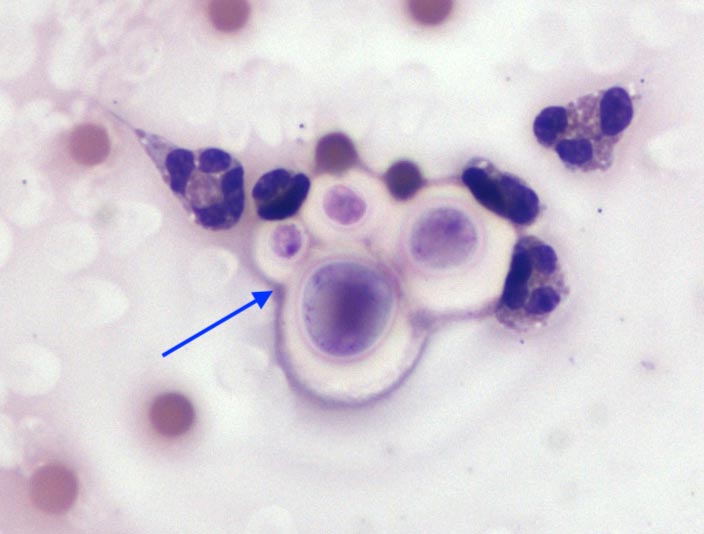
Figure 1 (main and below). Photomicrographs of the CSF of a dog with neurological signs; Wright-Giemsa 50×-100×.
The pictures in Figure 1 are from CSF collected from the cisterna magna of an adult male dog that presented with a four-day history of acute cervical hyperaesthesia and neurological deficits on the frontal limbs.
 MRI showed a diffuse intramedullary hyperintensity affecting the cervical and thoracic regions. What is your diagnosis?
MRI showed a diffuse intramedullary hyperintensity affecting the cervical and thoracic regions. What is your diagnosis?
The cytospin preparation showed a mixed population of nucleated cells, the majority being eosinophils, characterised by the presence of typical intracytoplasmic orange granules (pink arrows). A lower percentage of macrophages with abundant, vacuolated foamy cytoplasm (black arrows), and a few small lymphocytes were also noted. A few yeast forms were also evident, with a distinctive non-staining, thick, mucoid capsule surrounding a granular basophilic internal structure, compatible with Cryptococcus species (blue arrow).
Eosinophilic pleocytosis due to Cryptococcus species infection.
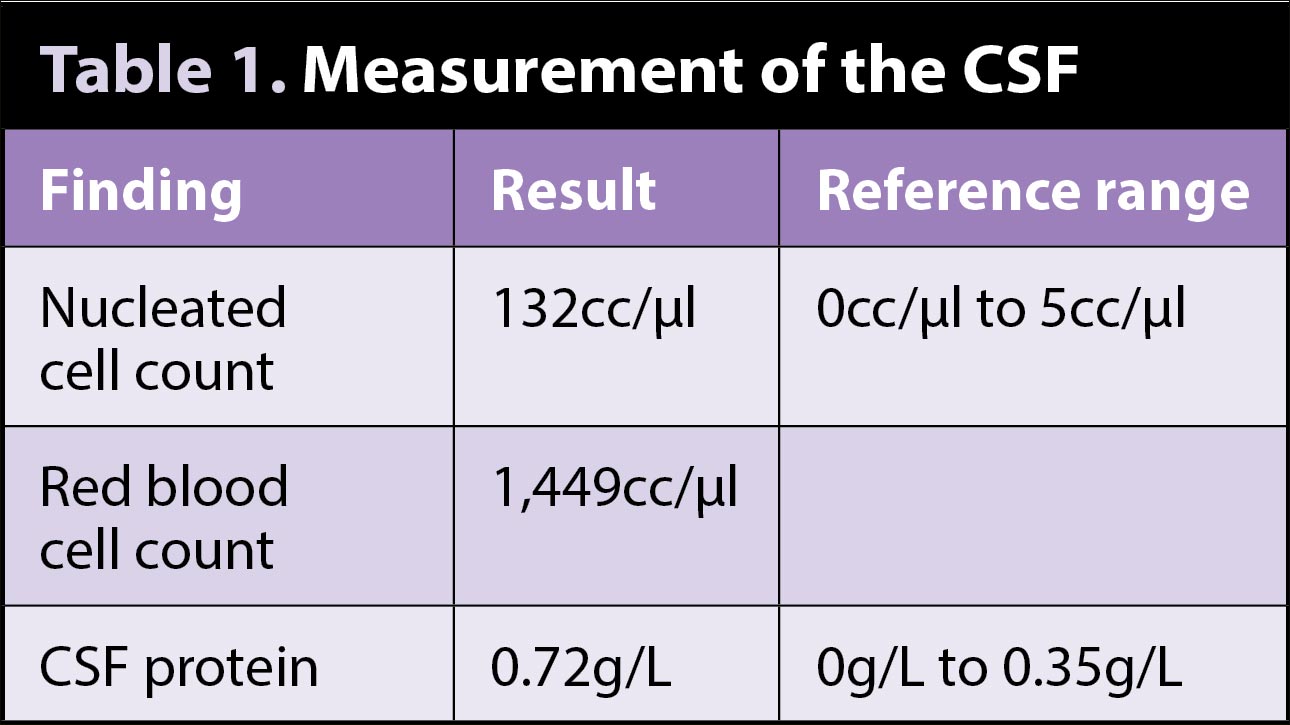
The submitted CSF is characterised by an increased percentage of nucleated cells, mostly eosinophils and macrophages, which are indicative of an inflammatory process. When specifically involving the CSF, the inflammation is referred to as “pleocytosis”, from the pleion “more”. Eosinophilic pleocytosis has been documented in idiopathic eosinophilic meningoencephalitis, infection processes, including those caused by Cryptococcus species, granulomatous meningoencephalitis, and rarely in cases of canine distemper and rabies virus.
Cryptococcus species are a large genus of dimorphic fungi, with a predilection for the CNS tissue. They frequently present as a disseminated disease with CNS and/or ocular involvement, and may result in mass lesions, meningitis or pseudocyst formation. CSF analysis typically shows pleocytosis, which can be variably neutrophilic, eosinophilic, mononuclear or mixed.
Serological and molecular methods may be helpful when the organism is not observed on cytology, and can be tested on serum and/or CSF samples.
The dog received fluconazole and amphotericin B and remained on gabapentin, tramadol, methocarbamol and anti-inflammatory doses of prednisolone. Despite therapy, the dog continued to deteriorate and was euthanised three weeks after diagnosis.