9 Nov 2015
Ariane Neuber
Job Title
Figure 2. Interdigital erythema in a dog with atopic dermatitis complicated by a secondary Malassezia dermatitis.
Skin diseases are commonly encountered in small animal practice (Hill et al, 2006) and can cause a lot of headaches for vets, owners and, in the case of ear disease, literally for the patient as well.
After routine reasons for visiting the vet – such as vaccinations, neutering and worming – skin diseases account for a large percentage of visits to the practice. If dealt with in a way where the client feels dissatisfied, it also often leads to practice hopping. However, if managed successfully, it can boost client confidence and loyalty.
A thorough approach to the case, leading to a firm diagnosis and development of an effective treatment plan, is essential to achieve good quality of life and client satisfaction. An important part of this is also good communication skills on the vets’ part, to set client expectation straight with regards to what can be achieved and to ensure optimal compliance. Many aids, such as client handouts, can be helpful in this process.
In this article, three common dermatological conditions – pruritus, otitis and pyoderma – and their management will be discussed.
Pruritus (Figure 1) is probably the most commonly encountered presenting sign for dermatological cases in small animal practice. It can be caused by a large number of diseases, but is most commonly associated with allergic (Figure 2), parasitic (Figure 3) and infectious diseases (Figure 4).




Less common diseases include autoimmune diseases such as pemphigus complex, metabolic disease such as hepatocutaneous syndrome and neoplastic conditions such as epitheliotropic lymphoma.
Discussion of the rarer condition is beyond the scope of this article and readers are referred to the textbooks. However, on the premise common things are common, it is more important for the general practitioner to be able to effectively manage allergies, parasitic diseases (which can be treated with parasiticidal agents) and common skin infections.
A combination of five satisfied criteria has a sensitivity of 85% and a specificity of 79% to differentiate dogs with atopic dermatitis from dogs with chronic or recurrent pruritus without atopic dermatitis. Adding a sixth fulfilled parameter increases the specificity to 89%, but decreases the sensitivity to 58%.
Before discussing management of allergic skin conditions with owners, it is important to be sure the patient has been diagnosed correctly and all other differential diagnoses have been ruled out. This sounds logical, but a surprising number of patients are treated for allergic skin conditions with other options not necessarily having been explored in detail.
Use of laboratory packages designed for pruritic animals, which include serum allergy testing, can sometimes lead to misuse of this test. Serum allergy testing, or any allergy test for that matter, is not a test to diagnose the disease, but only a means of formulating therapy, namely immunotherapy, or for allergen avoidance. If allergen-specific therapy is not going to be pursued it is probably not money well spent to even perform allergy testing.
Studies have shown in a large percentage of dogs without clinical signs compatible with atopic dermatitis (AD), allergen-specific IgE can be demonstrated and positive reactions can be obtained in intradermal allergy testing. The diagnosis is therefore a clinical one. Favrot et al (2010) published criteria helpful in reaching a diagnosis (Panel 1). In addition, it is important to methodically rule out other differentials by performing adequate diagnostic tests, such as cytology and skin scrapings, or trial therapy, for example, sarcoptic mange. Once an AD diagnosis has been reached, management concentrates on a few factors.
Good, year-round ectoparasite control is helpful in AD patients for various reasons – namely because, according to the threshold theory, added irritation would push a well-controlled patient over the pruritus threshold and because individuals already suffering from one allergy are genetically more likely to develop flea allergic dermatitis if periodically exposed to fleas. Due to many skin disease patients being maintained on shampoo therapy, systemic flea control is probably more effective as many other products are removed by frequent bathing to a large extent. Shampooing can be an important part of controlling secondary infections, the second aspect of controlling flare factors.
Oral essential fatty acids, topical essential fatty acids, essential oils or complex lipid mixtures, shampoo therapy or other topical preparations (sprays or mousses) are in this group of treatments. Although monotherapy with oral essential fatty acids (either as a supplement or enriched diet food) is unlikely to be sufficient to control most AD cases (Thierry et al, 2010) it can reduce the requirement for other treatments, including having a glucocorticoid sparing effect.
Studies have shown encouraging results with topical essential fatty acids, essential oils and complex lipid mixtures and, in the right patient, can be important as part of the overall treatment regimen.
Shampoo therapy is helpful as it reduces the amount of allergens, microorganisms and their by-products and inflammatory cells and their by-products, and it rehydrates the skin. However, frequent bathing might also dry skin and conditioners can be helpful in reducing this.
Medicated shampoos are available to control signs of seborrhoea and secondary infections without use of antibiotics. Bathing frequency depends on factors including the owner’s ability and the nature of the patient’s dermatological changes.
Systemic antipruritic/anti-inflammatory therapy includes the use of glucocorticoids (for example, oral prednisolone or methylprednisolone and topical glucocorticoid preparations), calcineurin inhibitors (ciclosporin, acrolimus, pimecrolimus) and Janus kinase inhibitors.
Given the lifelong nature of AD, oral glucocorticoids should be reserved for seasonal cases with only a short allergy season, cases in which no other medication can deliver good quality of life, due to financial restraints, or as a short-term measure, either to bridge the induction phase of calcineurin inhibitors or to treat short flares once factors such as a microbial infection or ectoparasite infestation have been ruled out.
Calcineurin inhibitors can be used successfully for long-term control of AD. A short course of glucocorticoids can be useful in the induction phase as satisfactory control of the clinical signs can usually only be expected after four to six weeks.
Once this has been achieved and the patient has been stable for a period of time, a dose reduction can be tried by either extending the dosing interval or reducing the daily dose, with the former method probably being more cost-effective if using capsule formulations.
Allergen-specific immunotherapy (ASIT) is the administration of rising doses of allergens identified in an allergy test to be specific for the individual patient with clinical AD.
Various studies have shown good efficacy of this form of therapy in a large number (50% to 80%) of patients treated for 6 to 12 months with ASIT. It is the only form of therapy that can actually change the course of the disease and prevent development of clinical signs after allergen exposure.
A study into client perception of different interventions commonly used for the management of AD (Dell et al, 2012) revealed clients perceive antihistamines to be beneficial as part of the management programme for their dog. About a third of patients seemed to improve to some degree following dietary changes and the only treatment that can achieve a true clinical remission in some patients is allergen specific immunotherapy.
Giving the owner a detailed prognosis – that is, making sure he or she understands his or her dog suffers from a lifelong condition that can be managed, but not cured – is important to improve client satisfaction.
The clinician in charge of the case must be a good detective to correctly diagnose the disease, have good communication skills, be aware of intervention that is evidence-based and be able to personalise the management programme for each individual patient/client constellation.

Otitis (Figure 5) is another common complaint in small animal general practice, is similar to allergic skin conditions resulting in pruritus (due to the fact the underlying disease is commonly an allergy) and is also often chronic, relapsing and lifelong.
Anyone who has suffered from ear disease can attest to the intense pain it can cause. Although most cases of uncomplicated otitis usually readily respond to therapy, with combination drops containing antibiotic, antifungal and anti-inflammatory components, the disease tends to relapse.
It is therefore important to identify and treat the primary disease (most commonly an allergy), the perpetuating factors such as chronic inflammatory changes, the predisposing factors (which the patient has been born with, so they are not treatable) and the secondary factors (microbial overgrowth/infection – usually Staphylococcus pseudintermedius or Malassezia pachydermatis; other bacteria such as Pseudomonas aeruginosa can also be involved; Table 1).
Treatment needs to incorporate a short-term plan to achieve remission of the acute episode of disease and make the patient more comfortable. However, a long-term plan also needs to be put in place, which includes investigation and management of the primary disease, reversal of secondary changes sustained and making the ear canal a less favourable environment for microorganisms to grow.
Cytology is essential to identify the microorganism involved and if rods are seen, bacterial culture is needed to identify which
rod-shaped organism is present, as bacteria such as Pseudomonas are often multi-resistant and require more aggressive treatment. In those severe cases, the patient also benefits from video otoscopic ear flushes, which are most likely available in referral practices only.

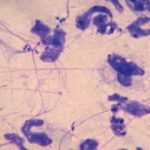
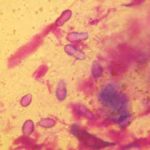
Skin infections are commonly encountered in small animal practice. The most important diagnostic test when an infection is suspected is cytology to identify the nature of the infection – for example, bacterial (Figure 6) or yeast (Figure 7) infections.
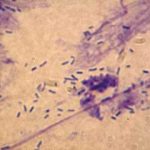
If bacteria are present, it is important to distinguish between cocci and rods (Figure 8). The latter usually warrant culture and sensitivity testing – particularly if found in an ear.
Recurrent bacterial skin infections are an area of dermatology that can be frustrating for owners and vets. In the interest of antibiotic stewardship, use of antibiotics should be restricted to cases where bacteria have been demonstrated – for example, on cytology or bacterial culture and with lesions too severe and widespread to respond to topical therapy alone.
If a course of antibiotics is indicated, it should be given for an appropriate duration at an adequate dose and the importance of compliance needs to be stressed to the client. Fluoroquinolones should be reserved for Gram-negative infections, but antibiotics such as cephalexin, amoxicillin clavulanate or cefovecin are all suitable choices.
Bacterial infections are usually secondary to a primary disease, much like for cases of otitis, and this needs to be investigated. Many of these patients are allergic, but endocrine diseases, ectoparasites and primary keratinisation disorders can also be the underlying disease, so a thorough work-up of each case is important and, as with all dermatology cases, good client communication is paramount to improve the chances of a successful outcome.
In summary, common dermatological diseases need to be approached in a methodical fashion. A firm diagnosis is required to be able to provide the owner with a realistic prognosis and put a tailored treatment programme in place for the patient. Many cases benefit from the input of a specialist dermatologist to optimise management of these patients.