15 Jul 2019
Kelly Bowlt-Blacklock and James Warland consider situations where antibiotics are appropriate in patients undergoing surgery (part 3 of 3).

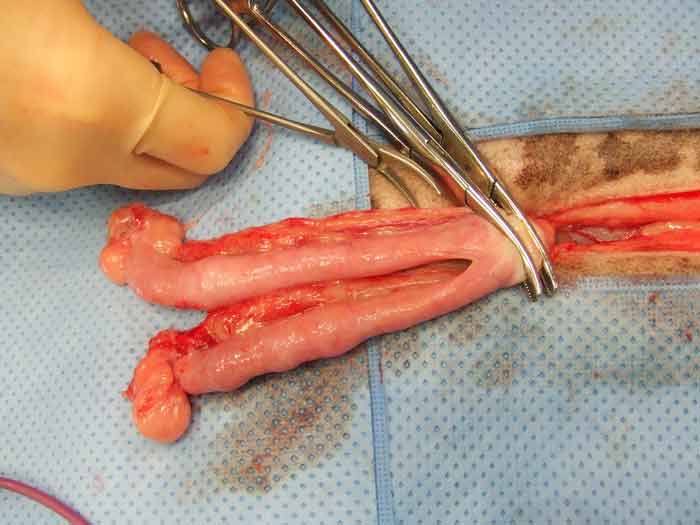
A wound over the carpus of a dog following a degloving injury and six days of negative pressure wound therapy. The site is completely covered in uniform, healthy granulation tissue, which is very resistant to infection. Antibiotics are not indicated.
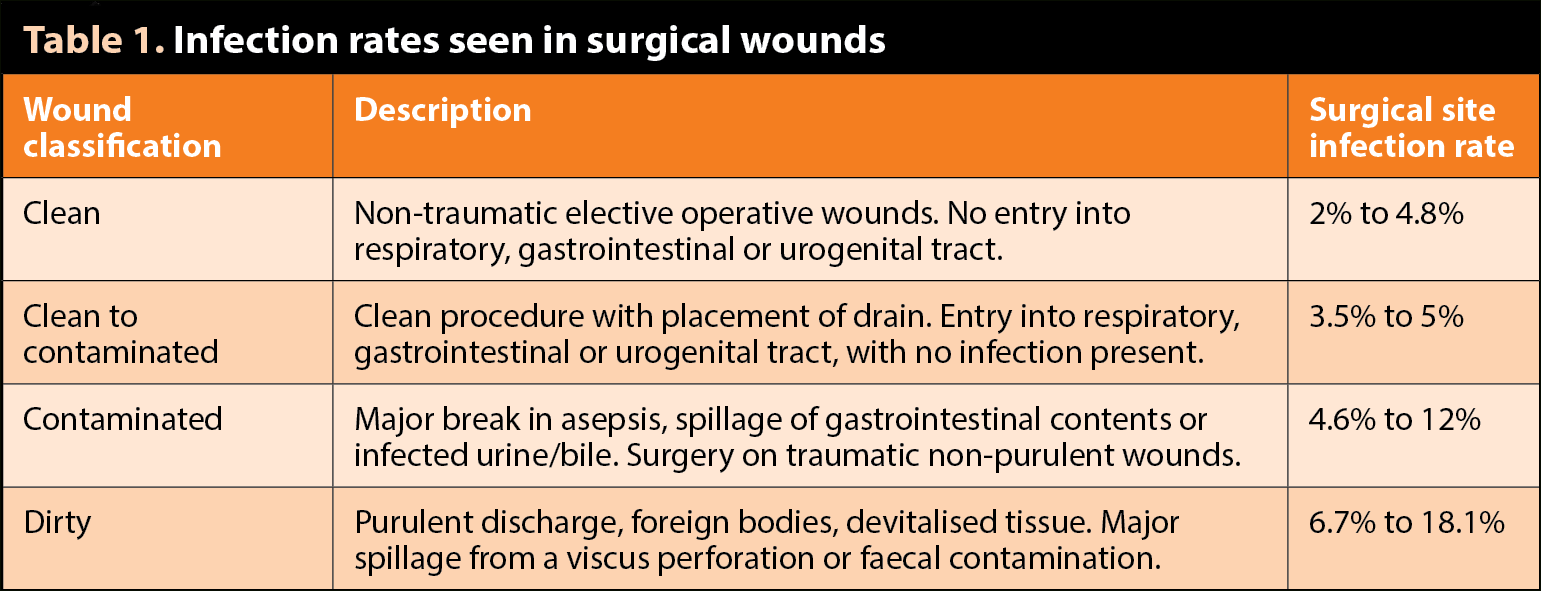
A surgical site infection (SSI) is one that occurs within 30 days of surgery (or 1 year if an implant is present)1, and depends on the amount and virulence of bacterial contamination, local wound conditions, and susceptibility of the patient (host).

SSIs are associated with significant morbidity, extended length of hospital stay, increased pain, increased or permanent complications, higher mortality and greater financial implications2,3,4.
A study in human health care on the efficacy of nosocomial infection control showed that well-organised surveillance and infection control programmes, including feedback of infection rates to surgeons, were associated with significant reductions in SSIs5,6,7,8,9. Such schemes have yet to be widely developed for veterinary hospitals10.
Scrupulous hand hygiene, meticulous adherence to Halstead’s surgical principles, strict asepsis, minimising staff numbers in the operating room, maintaining patient normothermia and outstanding postoperative nursing standards are the mainstays in preventing SSIs11,12.
The use of antibiotics to compensate for anything less than fastidious perioperative hygiene and surgical principles will not lower SSI rates, but will increase bacterial resistance and favour clinical adverse effects.
When considering the role of antibiotics in preventing infection following surgery, it is important to understand the following13:
Inappropriate antibiotic use (for example, unnecessary use of broad-spectrum antibiotics, excessively prolonged course, poor client compliance) results in increased risk of adverse effects and antibiotic resistance.
The use of prophylactic antibiotics should be based on careful risk assessment, including:
No antibiotics are required in healthy patients undergoing clean procedures (such as lump removal, castration, ovariohysterectomy and some splenectomies) of less than 90 minutes duration with no implant placement and where no obvious break in asepsis occurs17. In one study assessing dogs undergoing short-duration, clean surgical procedures, no difference occurred in SSI between patients given ampicillin compared with placebo18.
Prophylactic antibiotics may be indicated in patients undergoing prolonged (more than 90 minutes) clean or clean to contaminated surgical procedures (for example, laryngeal/tracheal surgery, vaginoplasty, gastrotomy, enterotomy), where infection would be catastrophic (for example, CNS, total hip replacement), where implants are used (still debated), where an obvious break in asepsis occurred, in contaminated wounds, or if the patient’s ASA grade is III to V.
For elective orthopaedic surgeries in dogs, one study showed antibiotic prophylaxis decreased SSI compared to placebo19. A second study showed SSI incidence was not different where antimicrobial prophylaxis was administered perioperatively over three hours or continued as a six-day course20. Contaminated wounds usually require antibiotics, but appropriate wound management should be prioritised.
Prophylactic antibiotics should be administered IV in time to ensure adequate tissue levels at the time of surgery and adequate tissue concentrations maintained until the wound has developed a fibrin seal (four to eight hours).
Appropriate prophylactic antibiotic selection must ensure an appropriate activity against the organisms likely to be present at that site will occur: usually this is clavulanic acid potentiated amoxicillin or a first-generation cephalosporin provided IV at anaesthetic induction and every 90 minutes thereafter until surgery is completed. Amoxicillin clavulanate administered IV is associated with a significantly higher incidence of adverse events (36%) compared with cefuroxime (2%) in dogs undergoing surgical procedures requiring prophylactic antibiosis21. Antibacterial administration after contamination is ineffective and increases the risk of SSI22.
Therapeutic antibiotics are indicated in dirty surgeries or where pre-existing distant or systemic infection has occurred. Antibiotics are often chosen empirically in the first instance, but bacterial culture and sensitivity is imperative for all dirty/contaminated sites and antibiotic choice should then be guided by the results obtained. Changing antibiotics without this information predisposes to multidrug-resistant infections. Therapeutic antibiotics may be necessary for several days (such as following dirty procedures – for example, septic peritonitis).
Concurrent and multimodal methods of wound decontamination and treatment (such as wound lavage, debridement, topical therapy – for example, honey or silver) are important and antibiotics are not required once a healthy uniform granulation bed has developed (which is naturally resistant to infection). Antibiotic application into the thoracic or peritoneal cavities is not appropriate.
The authors are grateful to Jeanette Bannoehr for her advice on the dermatology section, and Sarah Caddy for reviewing the manuscript. The AHT’s antimicrobial use policy was drawn up by the AHT’s infection control committee with guidance from the RVC infection control committee. The authors are grateful to both committees, particularly Rosanne Jepson for allowing the reproduction of sections from these policies in this article.