30 Jul 2024
Philip Witte outlines the different types of trauma to this region, and how to treat them.
Philip Witte
Job Title
A transarticular external skeletal fixator.
Trauma resulting in hock injuries is not uncommon in cats. Most frequently, this involves road traffic accidents.
Cats will present with all the usual signs of significant trauma, so life-saving treatments should be prioritised over the occasionally rather spectacular skin deficits and abnormal movement that clearly identify the hock as a target for veterinary attention.
Clipping/cleaning and support with the likes of splints may need to wait while the cat is stabilised. However, placing a support dressing with a sterile base layer in the first instance may be considered a part of the first aid, as it will reduce further contamination, minimise further damage to periarticular tissues and facilitate analgesia.
The feline hock has some specific anatomy that has an influence on the nature of hock injuries and their management. Readers with an interest in delving deep into the anatomy of the feline hock are directed to two excellent reports by Vollmerhaus et al published in Tierärztliche Praxis: Kleintierpraxis in 2002.
The vast majority of movement in the hock comes from the talocrural joint (estimated at around 90% in the canine hock, although this figure is not available for the cat).
The other joint levels consist of the calcaneoquartal and talocentral (together forming the proximal intertarsal joint), centrodistal, which is only present medially, and tarsometatarsal joints. These provide limited movement only.
The talocrural joint comprises a close fit between the two proximally directed talar ridges and three distally projecting ridges consisting of the medial (tibial) malleolus, the tibial cochlea and the lateral (fibular) malleolus. These five ridges interdigitate, giving the hock a somewhat constrained hinge-like function.
The distal tibia and fibula are connected by a stretch of fibrous tissue known as the distal tibiofibular ligament. Therefore, medial and lateral translation is prevented by the bony contours of the joint.
The talocrural joint is further stabilised by collateral ligaments. The canine hock has a single long and two short parts medially and laterally. The long parts are taut when the hock is extended (and are at most risk of traumatic injury in the dog), while the short parts are taut when the hock is flexed.
However, in the cat, the long parts are not present. They are considered to be replaced by what were reported by Vollmerhaus et al (2002) to be “contractile tension ligaments”.
Inserting on the base of the second metatarsal bone and proximal fifth digit medially and laterally, respectively, are the tendons of insertion of the caudal tibial and fibularis brevis muscles.
Muscles originate on the proximal fibula. Their tendons of insertion are long and narrow, and have fibrous attachment to the bones and soft tissue structures of the pes at various levels. They are also constrained within grooves in the malleoli, maintaining their position (and, thus, tension) through a full range of motion.
They were previously considered to provide valgus and varus rotational movements in the frontal plane in the talocrural joint. However, more recently, their function was recognised as important stabilisers of the hock in cats during extension. They were described as contractile tension ligaments, because they act to replace the long collateral ligaments present in dogs and, owing to the presence of a small amount of muscle at their proximal ends, may confer a little more control to the support structures of the feline hock.
As is the case in the dog, the short parts of the medial and lateral collateral ligaments are divided structurally in two: the short part of the lateral collateral ligament exists as fibulotalar and fibulocalcaneal parts, while the short part of the medial collateral ligament exists as a tibiotalar and tibiocentral parts.
The importance of these structures in cats has been investigated in a cadaveric study (Martin et al, 2022). The medial collateral ligaments (tibiotalar and tibiocentral) prevent excessive valgus deviation and pronation, while the lateral collateral ligaments (fibulocalcaneal and fibulotalar) prevent excessive varus deviation and supination.
Cats may present following trauma with a hock that appears to swing in the breeze. Rotational movement in the frontal plane of the feline hock should be reasonably tightly limited by the collateral ligaments (Nicholson et al, 2012).
The mechanism of traumatic failure of the collateral ligaments involves application of varus or valgus strain during (mostly) road traffic accidents. If the traction exceeds the elastic limit of the ligament(s), rupture will result.
If the resulting force is applied primarily to the bone from which the ligament(s) originate – that is, the malleoli – avulsion fracture will be the result instead of ligament rupture.
The factors that determine whether a trauma results in ligament rupture or malleolar fracture are not clear. Injuries may involve trauma to the medial collateral ligaments (or malleolus), lateral collateral ligaments (or malleolus) or may be bilateral.
One study of malleolar fractures revealed injuries affecting the medial malleolus in 5 out of 30 cats, the lateral malleolus in 10 out of 30 and fractures of both malleoli in 15 cats (Roch et al, 2009). Following failure of the collateral constraints, the talus is free to luxate from the tibial cochlea and fibular malleolus when the talocrural joint is flexed to 90°.
The talus will luxate medially with medial collateral rupture and laterally with lateral collateral ligament rupture. This explains the commonly recognised severe deviation of the paw on presentation or during examination.
Examination of a cat’s hock may be performed with the hock in 115° extension (a normal standing angle). It is of relevance to examine a dog’s floppy hock in flexion and extension to determine which combination of short and long parts of the collateral ligament(s) have failed, since this has a bearing on the surgical options. However, in the cat, the absence of a long part makes this of less relevance.
Radiography is used to determine the extent and location of injury or injuries (Figure 1).


Figure 1. Mediolateral (1a) and caudocranial (1b) radiographic views of the left hock revealing luxation of the talocrural joint in association with fracture of the fibular/lateral malleolus and presumed rupture of the medial collateral ligament.
Orthogonal views of the hock should always be acquired. Stressed views may be of use firstly to identify instability – particularly in the absence of malleolar fractures, which are usually very apparent radiographically – and secondly to open up subtle malleolar fracture gaps, to confirm a diagnosis of fracture.
Stressed caudocranial views (that is, valgus and varus stress, as in Figure 2) are likely to give more useful information than flexion and extension in the mediolateral view. However, the latter may also be useful – for example, to identify talocalcaneal luxation and other concurrent injuries.

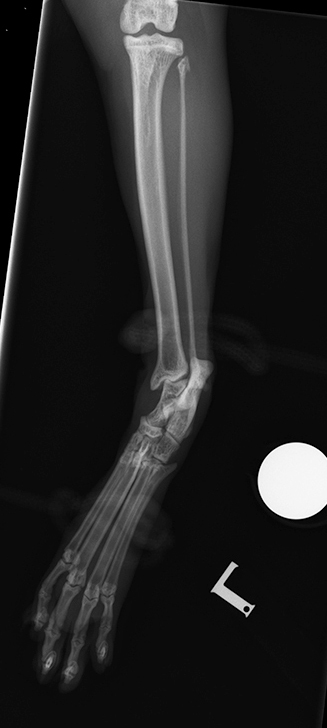

Figure 2. Neutral and stressed caudocranial radiographic views of the hock are used to determine the presence and severity of mediolateral instability. Figure 2a shows caudocranial view of left hock of a cat demonstrating soft tissue swelling in the region of the hock and no other abnormalities. Figure 2b shows same caudocranial view with application of varus stress through ropes applied to the crus proximal to the hock and to the metatarsus, demonstrating widening of the gap between the distal tibia and fibula, and opening of the tibio-talar joint space laterally. This finding may be consistent with failure of the distal tibiofibular ligament. The integrity of the lateral collateral ligament is uncertain. Figure 2c shows same view with application of valgus stress revealing opening of the tibio-talar joint medially. This finding is consistent with failure of the medial collateral ligament.
The surgical approach to the feline floppy hock can involve a combination of:
Attempts to perform primary repair of ruptured collateral ligaments are unlikely to be successful, since these structures are fine and have poor suture-holding characteristics. However, we can restore ligament function where sufficient bone stock is available to reattach malleolar fragments.
Such repairs will inevitably involve small pins and wires in small (potentially brittle) fragments of bone. Therefore, augmentation of such a repair is often warranted. Regardless of whether primary repair (of ligaments or avulsion fragments) is performed, further surgical augmentation/stabilisation of the hock is likely to be required.


Figure 3. Anatomical specimen annotated to demonstrate locations of origins and insertions of medial (a) and lateral (b) collateral ligament prostheses. Bone tunnels are drilled using a 0.5mm to 1mm Kirschner wire or drill bit, and fine suture (slowly absorbable or non-absorbable) is passed between them. In practice, placing these prostheses is complicated by the difficulty with creating viable bone tunnels in small bones without disrupting other structures, and passing the suture is also difficult, requiring patience and dexterity. The medial landmarks are the medial malleolus, the head of the talus (near the talocentral joint) and the body of the talus (just distal to the malleolus on the medial aspect of the talar trochlea). The lateral landmarks are the lateral malleolus, the proximal and distal extents of the calcaneus.
Prosthetic collateral ligament replacement involves the use of monofilament non-absorbable suture material through bone tunnels (Nicholson et al, 2012) or using suture screws/anchors to replicate the origins and insertions of the failed short parts of the collateral ligaments (Figure 3). Thus, for a medial instability (that is, increased range of motion to valgus stress) the landmarks are from the medial malleolus to the head and body of the talus. For a lateral instability, the landmarks are from the fibular malleolus to the proximal and distal extents of the calcaneus.
Objective data regarding clinical outcomes for this technique have not been reported. Internal fixation of talocrural luxation using ligatures was reported by Schmökel et al in 1994 and 2001, revealing a poor long-term functional outcome.
A biomechanical study of knotted versus knotless stabilisation techniques for replacement of the feline medial collateral ligament was published in 2019 by Luescher et al, suggesting some groups were still invested in attempts to improve outcomes with internal fixation.
Attempts to place prosthetic ligaments where significant skin deficits are present is not recommended.
The purpose of temporary immobilisation of the hock is to allow periarticular fibrosis to stabilise the joint. While the latter option would be expected to result in a poor outcome for a dog, it is remarkable how stability in a cat’s hock can be restored through periarticular fibrosis alone.
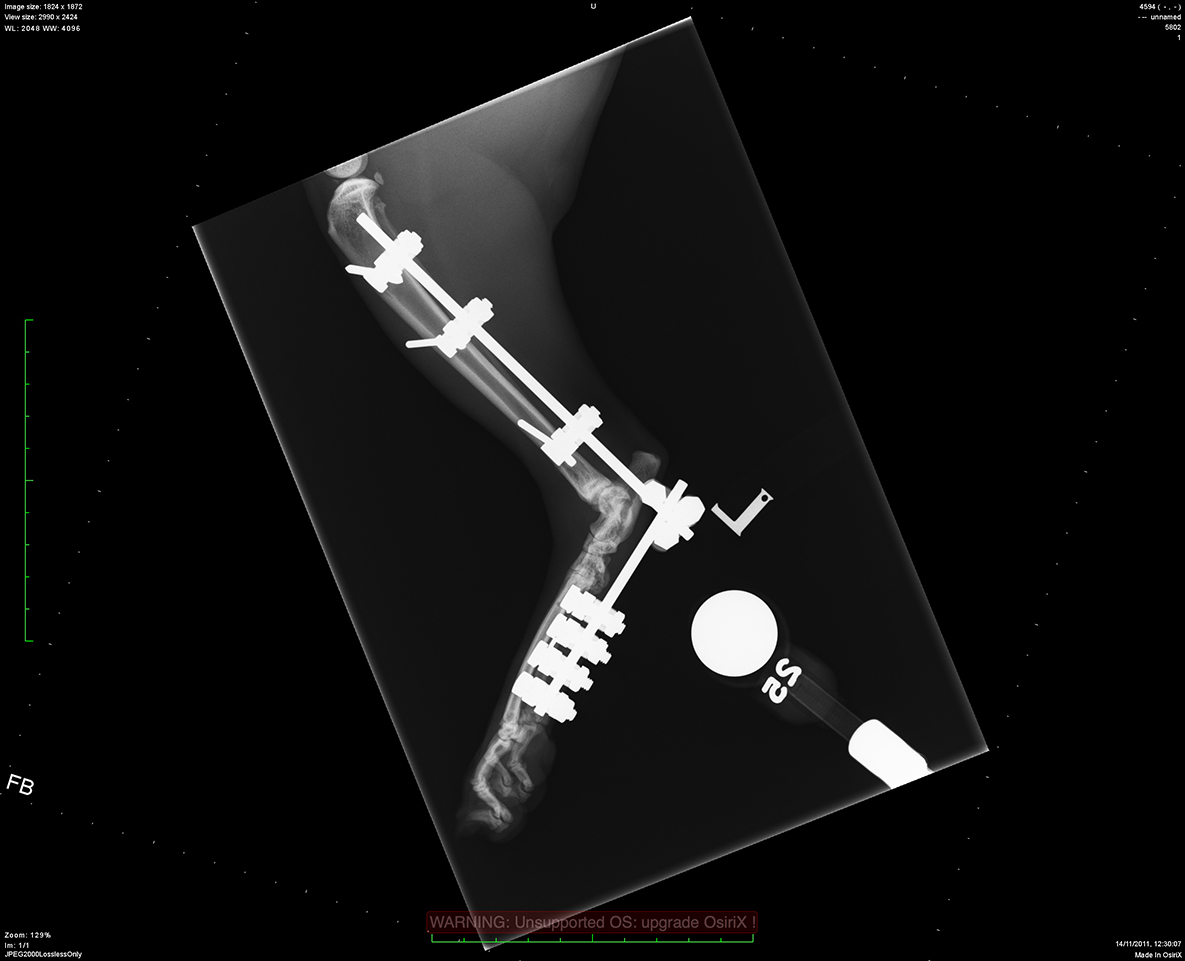
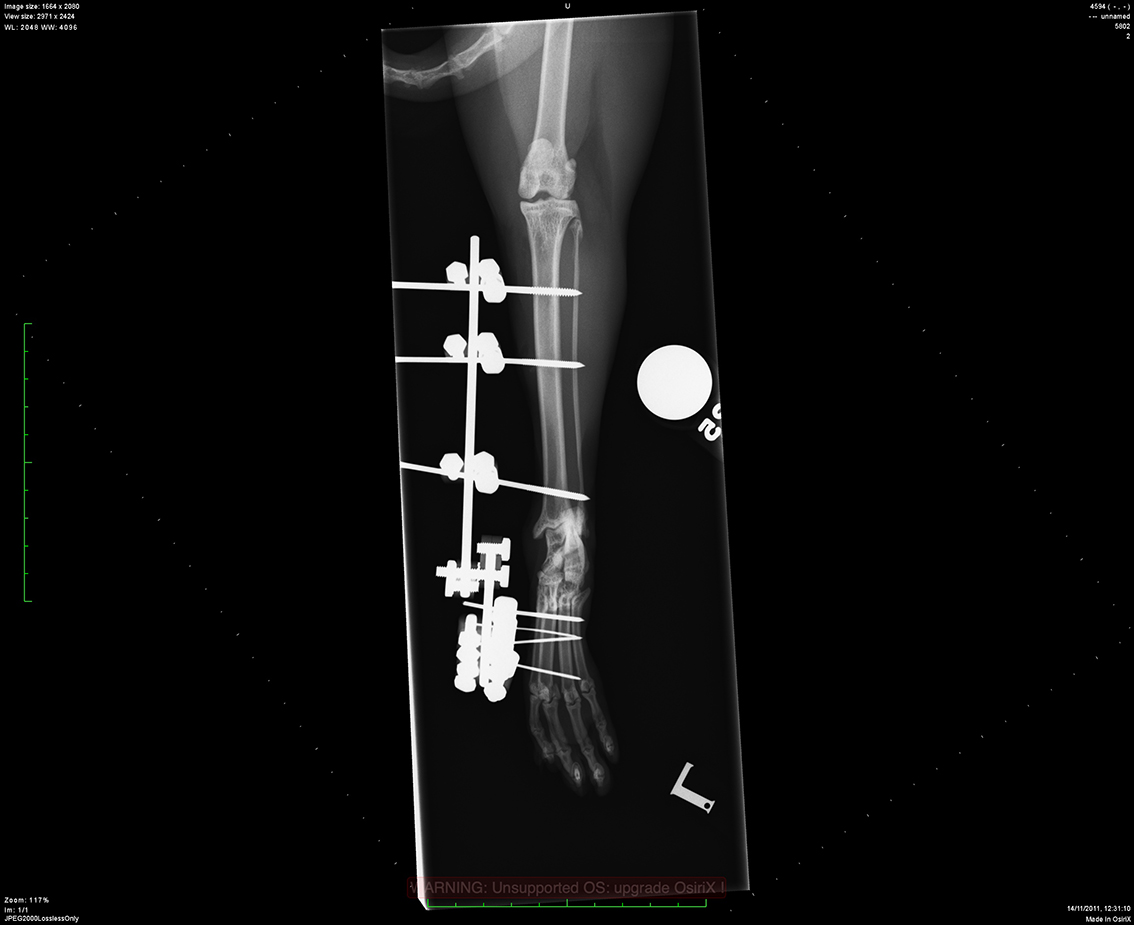
Figure 4. Mediolateral (a) and caudocranial (b) radiographic views of the left hock of a cat with luxation of the talocrural joint associated with medial and lateral collateral ligament ruptures. A transarticular external skeletal fixator has been applied with 1.6mm positive profile end-threaded fixation pins in the tibia, and 1.2mm and 1mm positive profile end-threaded fixation pins in the metatarsus. The frame is a modified type 1 frame in that the connecting rods are located on one side (medial) and the pins are all half pins. Fixation elements in this case are mini clamps including a double clamp to connect the two connecting rods. A large variety of modifications of this approach are possible, including placing fixation pins into the calcaneus or tarsal bones, using bilateral fixation (that is, a connecting bar medially and laterally) and use of other fixation systems, including acrylic/putty connecting bars.
The technique involves rigid immobilisation for four to six weeks using a transarticular external skeletal fixator (Figure 4). However, less rigid immobilisation with external coaptation has also been performed (the reduced stiffness in the immobilisation theoretically will result in a less stable joint in the long term, and external coaptation carries its own complications in terms of skin damage and intolerance by the feline patient).
In outcome studies published in the past few decades, temporary immobilisation appears to be the preferred technique. Outcomes were reported by Kulendra et al (2011) and Yardimci et al (2016), with subjectively good results. Remobilisation of the joint is recommended before six weeks, since evidence suggests that immobilisation of a joint for greater than six weeks will result in irreversible damage to articular cartilage. Hock immobilisation can be helpful for management of skin deficits, including in cases requiring free skin grafts.

Traumatic injury to the calcaneoquartal and talocentral joints is not common in the cat. This injury may not be directly apparent on radiographs; however, soft tissue swelling in the region should indicate this as the site of concern, and this is a situation in which a stressed radiographic view (hyperextension in the case of Figure 5) may reveal the injury.
The injury may be dorsal or plantar, or both. In cases of dorsal instability, conservative management is reasonable, since the plantar surface is the tension surface of the joint. However, a failure for lameness to resolve within two to four weeks is an indication for intervention.
Fixation may involve use of a small lateral plate with screws in the calcaneus (2mm or 2.4mm) and fourth tarsal bones (1.5mm, or 2mm in a large cat). The loading of this implant on its side will increase the area moment of inertia such that stiffness should be sufficient, despite the relatively small size.
A more familiar approach may be to perform partial tarsal arthrodesis (that is, application of a plate extending from the proximal calcaneus to the distal third of the metatarsus, giving more bone stock distally for implant fixation into the metatarsal bases).
Tarsometatarsal luxation is not uncommon (Figure 6). Two methods of fixation are available. A lateral plate may be placed, to perform partial tarsal arthrodesis, or pins may be inserted normograde from slots burred into the dorsal aspect of the distal metatarsal bones (particularly the third and fourth) and driven proximally to bridge the tarsometatarsal joints.
During this procedure, and during application of screws from medial to lateral or lateral to medial across the metatarsals, it is important to note these bones are not arranged in a single plane, with the third and fourth metatarsal bases located somewhat obliquely dorsal to the second and fifth, such that an attempt to drill across all four metatarsal bases from one side to the other will not be successful.
A familiarity with the arrangement of these bones facilitates greatly the reduction and fixation of luxation at this level.

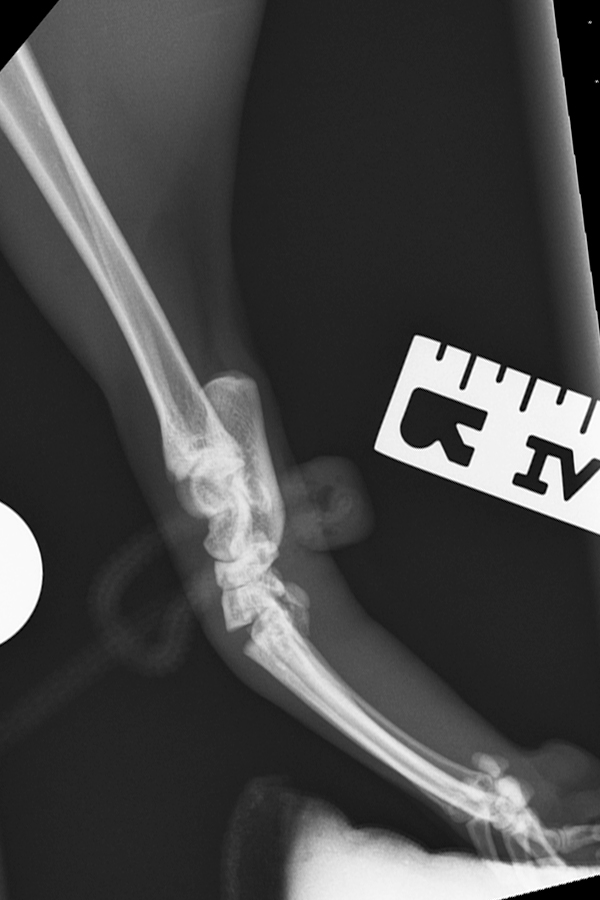

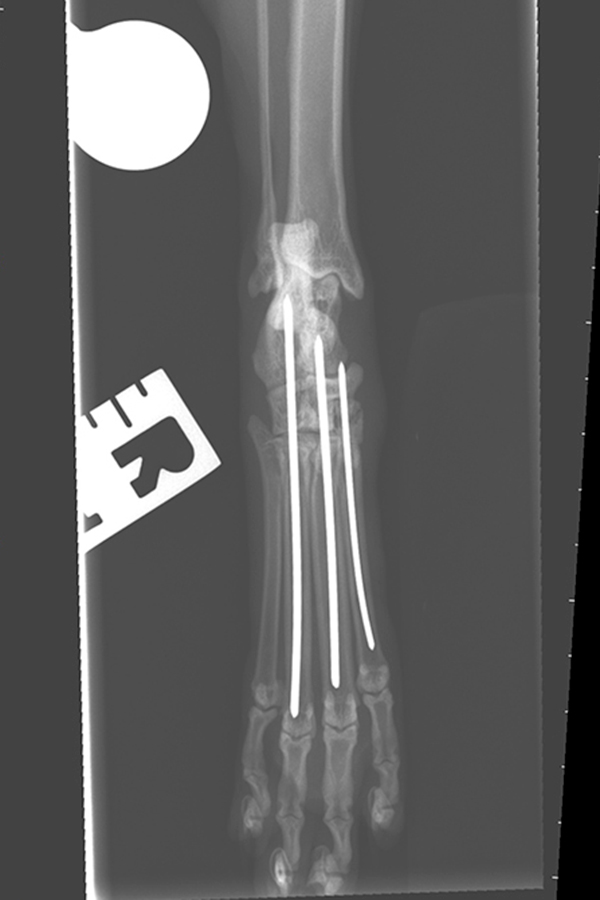
Figure 6. A mediolateral view of the right hock of a cat reveals a suspicion of an increased tarsometatarsal joint space (6a). When stressed into hyperextension, tarsometatarsal luxation becomes apparent. In a different case (6c) more obvious tarsometatarsal luxation is present in the neutral view, with a widened joint space and a suggestion of dorsal translation of the metatarsal bases with respect to the numbered tarsal bones. Figure 6d reveals narrow gauge wires have been introduced through slots in the distal second, third and fourth metatarsal bones, and these have been driven proximally across the luxated tarsometatarsal joints (and in the case of the third and fourth metatarsals, they have also been driven across the proximal intertarsal joints).
Talocalcaneal luxation (Figure 7) involves rupture of the two talocalcaneal ligaments. The talus remains with the tibia. However, the calcaneus remains in contact with the remainder of the hindpaw through an intact calcaneoquartal joint.
Sometimes, talocentral luxation occurs, and less frequently calcaneoquartal luxation occurs in association with this injury.


Figure 7. A mediolateral neutral radiographic view of the left hock of a cat demonstrate luxation of the talocalcaneal and talocentral joints (7a). Significant displacement is not evident and the medial and lateral collateral ligaments remain in tact. Therefore a single 1.5mm screw was used to reduce the talus to the calcaneus (7b). An understanding of the anatomy at this level is important, since visualisation of the calcaneus into which the screw is driven is limited.
Calcaneal fracture in cats as a result of trauma is not reported, though is observed occasionally, often in association with multiple hock injuries.
One technique in dogs involves driving an orthopaedic or Kirschner wire normograde from the proximal aspect to bridge fractures, often combined with a tension band wire. However, drilling into the narrow feline calcaneus may risk fracturing the bone further, so plating may be preferable.
With the advent of 1mm and 1.5mm implants, no calcaneus is too small to accept a plate. Plates are typically applied to the lateral surface. Given that the calcaneus has a dorsal compression surface and a plantar tension surface, a laterally applied plate will be loaded sideways on, maximising the area moment of inertia despite the small size of implant.
Talus fracture is a relatively frequent finding in cats with hock trauma. The talus fractures through the neck, that is, between the head (distal) and body (proximal portion which accommodates the talar ridges). Where fragments are sufficiently large, they can be fixed to the calcaneus with combinations of 1.5mm or 2mm screws and 1.1mm arthrodesis or Kirschner wires.
Central tarsal bone luxation (or fracture/luxation) is a relatively common finding in dogs, particularly sighthounds. However, this type of injury has been reported only once in cats in the veterinary literature (Cinti et al, 2016).
Fixation was with a single 2mm screw and two 0.8mm Kirschner wires. An alternative approach may have been to perform partial tarsal arthrodesis with a medial or lateral plate following reduction of the fracture.
One concern when presented with a patient with fractures of the cuboidal bones is that other small fractures may also be present, potentially limiting the functional outcome, in which case immobilisation of the entire pes from calcaneus to metatarsals (that is, partial tarsal arthrodesis) may be superior in terms of restoring comfort.
Two options are available for salvage in the feline hock: partial tarsal arthrodesis, in which the joints of the pes are immobilised but the talocrural joint is spared, and pantarsal arthrodesis, in which the talocrural joint is also fused.
Clearly, the indications for these procedures are different. Essentially, partial tarsal arthrodesis may be used to fix fractures and luxations between the calcaneus and the metatarsal bones.
The procedure involves placing a lateral plate with screws in the calcaneus, fourth tarsal and metatarsal bones. Removal of articular cartilage at the various levels is not considered vital in cats.
Partial tarsal arthrodesis may be argued to be overkill for some conditions; for example, a tarsometatarsal luxation. However, attempts to preserve the calcaneoquartal joint when performing fixation of a tarsometatarsal luxation may be frustrated (or tenuous) as a result of limited bone stock in cats.
Where no option exists of preserving the talocrural joint, we perform pantarsal arthrodesis. Although the indications for this procedure are talocrural salvage, the joints of the pes are also fused for two reasons: firstly, the limited motion joints could undergo excessive strain following arthrodesis limited to the talocrural joint, since they would be acting through a longer lever arm, potentially resulting in discomfort at these joint levels; secondly, because of a lack of bone stock if the tarsus and metatarsus are not included in the fixation.
Implants are available specifically for feline pantarsal arthrodesis (since the feline standing angle of around 115° means canine plates are not suitable), although application of veterinary cuttable plates has been reported.
The floppy hock (talocrural luxation) is associated with malleolar fracture or collateral ligament rupture.
The approach may involve fixation of the malleoli/collateral ligaments, but always involves consideration of augmentation with synthetic collateral prostheses or temporary immobilisation with transarticular external skeletal fixator.
Other injuries of the hock are addressed individually, though partial tarsal arthrodesis is a good option for restoration of comfort in a pes with various forms of trauma and an intact talocrural joint.