28 May 2024
Irina Matricoti shares the latest thoughts on this common aural disorder found in both cats and dogs.
Irina Matricoti
Job Title
Image © famveldman / Adobe Stock
Otitis externa is a very common condition in veterinary medicine, and it is defined as an inflammatory process of the inner pinna and/or the external ear canal, which is composed by a first portion – the vertical ear canal – and a deeper portion, the horizontal one, which ends at the tympanic membrane.
Inflammation might or might not be associated with infection. As the pathogenesis is often multifactorial, a detailed diagnostic procedure is necessary to identify all the causes that might contribute to its development.
An aetiological system of classification divides the factors involved into predisposing and perpetuating factors, and primary and secondary causes (known as PPSP). Causes and factors involved should be investigated and addressed to successfully manage otitis externa cases.
Are primary causes considered conditions that trigger otitis externa? Like the entire body skin, the ear canals are covered by stratified squamous epithelium, and consequently, the majority of the diseases that cause dermatological problems might affect the ears.
Primary causes include parasitic diseases (for example, Demodex species and Otodectes cynotis), allergic diseases (atopy and food allergy), primary keratinisation defects (such as idiopathic seborrhoea), secondary keratinisation defects (for example, consequent to hypothyroidism), foreign bodies (grass awns), drug reaction to topicals, glandular disorders (sebaceous glands hyperplasia and neoplasia), autoimmune diseases (such as pemphigus foliaceous and sebaceous adenitis) and viral infections.
When primary causes are not properly identified and controlled, this frequently incurs into recurrent episodes of otitis, namely any subsequent episode of inflammation/infection within three months of a previous episode that was completely resolved. Allergic diseases (atopic dermatitis and food allergy) are the most frequent primary causes of recurrent otitis externa. In atopic dogs, the inflammation is initially limited to the pinnae, external orifice or vertical portion of the external ear canal. However, it frequently progresses to involve the entire ear canal, and secondary infection is a common sequela.
Primary idiopathic seborrhoea might be a primary cause in breeds prone to this condition (such as the English springer spaniel, West Highland white terrier or basset hound). It causes an increased epidermal cell turnover that leads to an excess of cerumen accumulation and inflammation. Hypothyroidism also can cause seborrhoeic changes leading to ceruminous otitis.
Bacteria and yeast are not classed as primary causes, but rather secondary causes: they take advantage of a previous inflammation, microbiome alteration and/or cerumen accumulation caused by the triggering cause.
Microorganisms make up the normal ear microbiota, which is highly diverse and rich, and include several phyla. The most important microorganisms of the external ear are Malassezia pachydermatis, Staphylococcus pseudintermedius and Staphylococcus schleiferi. These are also the most frequent pathogens responsible of otitis. In recurrent chronic cases, other Gram-negative bacteria – particularly Pseudomonas species – might overgrow.
“To successfully manage otitis externa, therapy should address all the causes (primary and secondary) and the factors (predisposing and perpetuating) involved in its pathogenesis.”
Predisposing factors are those conditions that increase the risk of developing otitis. Usually, these factors alone are unable to cause otitis; however, they can contribute to its development, slow the healing process and favour relapses.
These factors include the conformation of the ear canal (for example, in the Shar Pei or brachycephalic breeds, which have usually stenotic ear canals due to skin folds or for the skull conformation), and higher density of ceruminous glands (for example, cocker spaniels), the excess of hair in the ear canal, or certain habits in some dogs (dogs that are frequently bathed or that attend swimming pools).
Perpetuating factors are all those conditions that prevent otitis resolution and lead to a progressive worsening of the disease. They are the result of pathological alterations induced by chronic inflammation and include stenosis of the ear canal due to epidermal and glandular hyperplasia, fibrosis and mineralisation of the ear canal cartilages. All these changes affect the normal epithelial cell migration.
In normal conditions, cerumen, composed by superficial cells and glandular debris, migrates from the tympanic membrane to the external orifice to be expelled, as a “self-cleaning” mechanism. Inflammation, especially if chronic, alters this mechanism inducing cerumen accumulation and, consequently, bacteria or yeast overgrowth.
Otitis media is another important perpetuating factor. In the middle ear, the ventral tympanic bulla acts as a reservoir of exudate, bacteria and toxins. This exudate is difficult to treat and often remains as a source for recurrent infections of the external ear canal. Perpetuating factors may be the major reason for poor response to therapy.
To successfully approach otitis externa, it is necessary to obtain accurate medical data to identify possible predisposing factors such as breed signalment; some habitats of the dog; and the age of the animals at first onset (for example, aged dogs and cats might suffer from neoplastic disease, while young dogs might suffer from atopic dermatitis).
If the owner reports several recurrent episodes of acute otitis externa, this presumably means that a primary cause, such as an allergic disease, has not been addressed, and sometimes these episodes might be seasonally recurrent. A careful clinical examination through an otoscope is necessary to evaluate the presence of primary or perpetuating factor (presence of polyps, mass, foreign bodies, stenosis of the ear canal, damage of ear drum, presence of hairs that might trap exudate and/or ceruminous gland hyperplasia), the presence of ulcerative lesions and the type of discharge (absent, ceruminous or purulent). If the inspection is painful, it should be performed under general anaesthesia. Palpation of the ear canal is necessary to evaluate the presence of mineralisation of the ear cartilages.
Mineralisation represents a chronic, irreversible change that must be taken into account before giving the client reasonable expectations about the prognosis. In any case of otitis, a careful dermatology examination of the entire body should be performed. Many primary diseases, such as atopic dermatitis, primary keratinisation defects, or endocrinopathies, often affect other body areas.
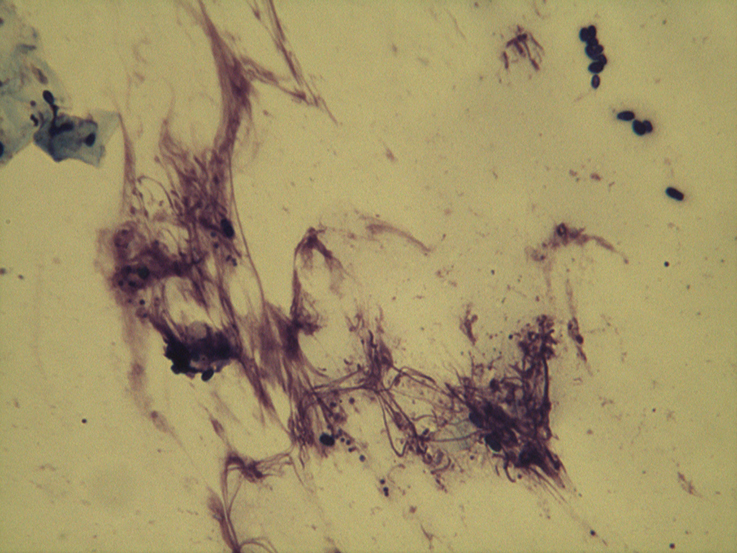
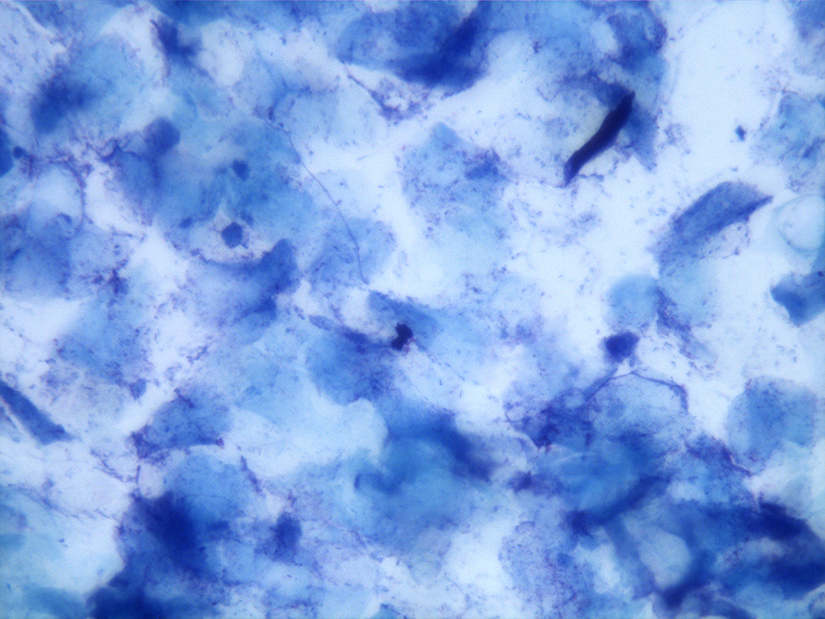
Lastly, skin scraping and cytology samples should be always collected to identify parasites, yeast or bacteria. The cotton swab is also useful to identify ear discomfort or pruritus in some dogs with only mild inflammation. Cytology might show neutrophils with intracellular bacteria indicating the presence of an infection (Figure 1), while the sole presence of numerous bacteria or yeast mixed with wax and epithelial cells is indicative of bacterial/yeast overgrowth (Figure 2), which might be mild to severe. In addition, cytology allows identification of the morphology of bacteria (cocci or rods). Rods, such as Pseudomonas, are most frequently associated with antibiotic resistance and with otitis media. Cytology must be performed at every recheck to asses resolution of infection.
Bacterial culture is not routinely performed in cases of otitis externa. It must be performed when antibiotic systemic therapy is indicated (concurrent otitis media or in cases of stenosis of the ear canal, which prevents the use of topical drugs) and whenever the possibility of antibiotic resistance to topical therapies is perceived, even if this is not frequent. Resistance to topicals is most frequently encountered with rods and in general with chronic otitis when several classes of antibiotic have been tried. However, bacterial susceptibility might not be predictive of the efficacy of topical treatments. In fact, even if the microorganism is classified as resistant, topical treatment can achieve very high concentration locally, showing clinical efficacy despite the result.
On the other hand, when sensitive, the result does not take into account some local factors (stenosis, hairs or biofilms) that can prevent antibiotic efficacy.
From this clinical approach, clinicians classify otitis externa mainly in three different types. Erythematous otitis usually shows only erythema, which can involve the entire external ear or be restricted to the sole pinna and horizontal canal (Figure 3). Discharge is absent and cytology is negative for infection, or might show a mild overgrowth of cocci or yeast.


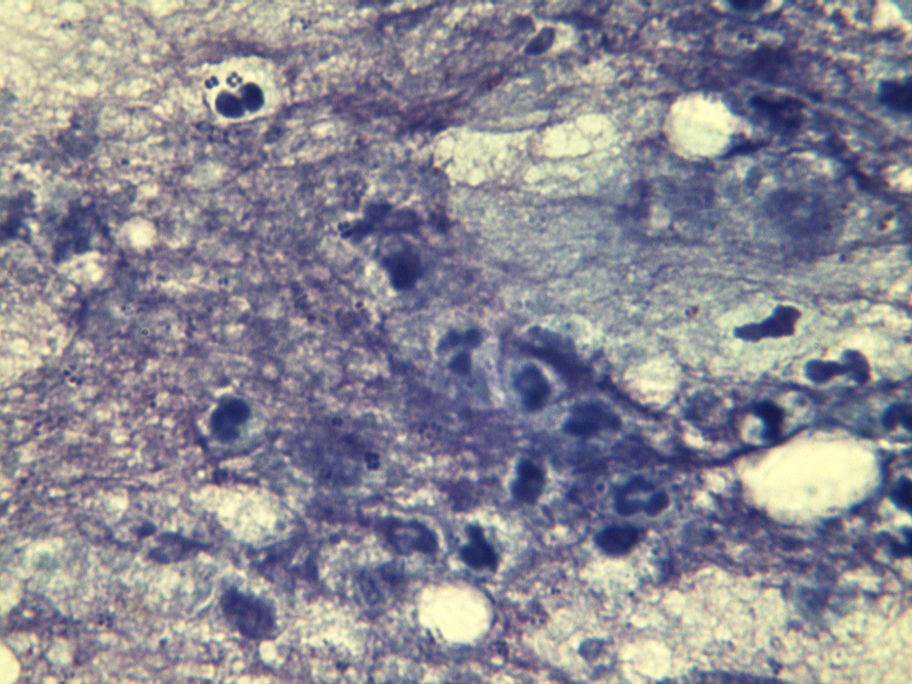
Erythematous otitis is often associated with atopy or food allergy. If left untreated, it might evolve into erythroceruminous or suppurative otitis and become chronic. Erythroceruminous otitis is characterised by inflammation, a more intense wax exudate and Malassezia or bacterial overgrowth (Figure 4). Suppurative otitis is characterised by abundant purulent discharge, erythema, occasional ulceration and numerous bacteria – inside and outside neutrophils (Figure 5).
Sometimes, it is possible to see suppurative otitis with yeast infection. Suppurative otitis is often complicated by the presence of biofilm (Figure 6). Biofilm is an aggregation of microorganisms embedded into an extracellular matrix that protects bacteria from the action of antibiotics and allows them to easily share the resistance gene, providing a reservoir of resistant bacteria. Otitis externa can become chronic, and it is characterised by visible stenosis of the ear canal, erythema, glandular hyperplasia, often lichenification of the pinna and, in extremely chronic cases, cartilage mineralisation.

To successfully manage otitis externa, therapy should address all the causes (primary and secondary) and the factors (predisposing and perpetuating) involved in its pathogenesis.
The first step usually consists in treating infection, removing excess of cerumen or exudate and resolving perpetuating factors. The second step is to control primary cause to avoid relapses, and if possible, eliminate predisposing factors. Cleaning the ear canal is pivotal in removing debris and secretions, which sequestrate pathogens and may inactivate medications. It is performed at home with variable frequency (from once daily to one or two times a week) depending on the amount of exudate. If exudate/cerumen persists and it is difficult to visualise the bottom of the ear canal, despite frequent home cleaning, ear flushing should be performed under general anaesthesia to remove debris.
The ear cleaning can be performed with cleanser or antiseptic. In the case of infection or pathogen overgrowth, antiseptics should be preferred. Mild microbial overgrowth may be managed with only topical antiseptic. Several antiseptics are found in ear products including isopropyl alcohol, aluminium hydroxide, chlorhexidine, iodine, parachlorometaxylenol, propylene glycol, sodium chlorite and sulphur. These agents are often combined with acids (acetic, boric, benzoic, lactic, malic and salicylic acids) to lower the pH.
Antiseptics have the advantage of being broad spectrum, do not promote resistance to antibiotics and might have synergistic effects when used in combination with antibiotics. Tris-ethylenediaminetetraacetic acid (EDTA) disrupts the cell walls of Gram-negative bacteria, rendering the bacterial cell more porous, and inhibits the effects of bacterial enzymes.
Tris-EDTA is useful in eliminating biofilm and might potentiate the action of some antibiotics (such as gentamicin, fluoroquinolones, silver sulphadiazine and chloramphenicol). N-acetyl cysteine is also found in association with tris-EDTA, acts against biofilm and is mucolytic. AMP2041, an antimicrobial peptide associated with Tris-EDTA and chlorhexidine, works by disturbing and perforating the bacterial walls.
In case of ceruminous otitis, ceruminolytic or ceruminosolvents should be preferred, which usually contain squalene, dioctyl sodium sulfosuccinate, carbamide peroxide, propylene glycol, butylated hydroxytoluene and cocamidopropyl betaine. Ceruminolytic/solvent products, with the exception of squalene, can cause ototoxicity in cases of a non-intact tympanic membrane, and they should be flushed with saline solution when used in those circumstances.
Topical antibiotics are used in cases of suppuration or moderate to severe bacterial overgrowth. Numerous topical preparations for the external ear canal are available on the market, with most being combinations of a glucocorticoid, an antibiotic and an antifungal.
Polymixin B, fusidic acid, florfenicol, gentamicin, enrofloxacin, marbofloxacin and orbifloxacin are suitable for most bacterial infections. Among these, fluoroquinolones, gentamicin and polymixin B are usually effective against Pseudomonas species. Ticarcillin, polymyxin B, neomycin, tobramycin and amikacin are potentially ototoxic, and should be used with care if the tympanic membrane is damaged. Florfenicol and gentamicin are available in a long-acting topical otic product.
The European Medicines Agency has categorised antibiotics for veterinary use in four classes, and clinicians should prefer antibiotics in class D rather than antibiotics in class C and B, and avoid antibiotic in class A. The antifungal ingredients contained in the majority of otic products are polyenes (nystatin), azoles (miconazole, posaconazole or clotrimazole) or allylamines (terbinafine). Other ingredients found in many cleaners have also been shown to have some anti-yeast activity.
Several glucocorticoids are found in ear drops, ranging from more potent agents (mometasone, hydrocortisone aceponate, fluocinolone, dexamethasone and betamethasone) to relatively less potent drugs (triamcinolone acetonide and prednisolone). The choice should be driven by the grade of inflammation of the ear canal and the risk of systemic absorption. With the exception of hydrocortisone aceponate and mometasone, all topical glucocorticoids may potentially cause adrenal suppression – especially when used for a long time.
“Clinicians must be able to identify factors and causes involved in any case of otitis, and each of them should be addressed…”
Systemic antibiotic therapy is indicated only in severe otitis externa where fibrosis and calcification have caused stenosis of the ear canal, which prevents application of topicals, and in case of otitis media. The choice of systemic antibiotics should be based always on culture and sensitivity test, especially when rods are visible at cytology and Pseudomonas species infection is suspected.
Systemic glucocorticoids are also used systemically at anti-inflammatory dosages, in severe ear inflammation and always when stenosis and hyperplastic changes of the ear canal are present. They inhibit hyperplasia and secretion of ceruminous glands, and reduce proliferative changes in the walls. Mineralisation and calcification are late modifications that cannot be reversed.
Treatment of perpetuating factors might take months and, after a course of oral steroids, a switch to a pulse therapy with topicals (such as hydrocortisone aceponate, which is not absorbed systemically), administered generally two to three times a week, is often necessary for a longer management. Otitis media, a frequent perpetuating factor, requires tomography and flushing of the middle ear in general anaesthesia by means of video-otoscopy.
Once infection has been resolved (usually in two to six weeks depending on the severity), efforts should be directed in controlling primary causes, otherwise otitis will relapse. Parasites, neoplasms and foreign bodies are usually easily identified at primary consultation, and resolved. Other primary causes might be overlooked.
If food allergy is suspected, a food trial should be proposed and continued after the complete cure of bacterial/yeast infection to evaluate efficacy of the diet in avoiding otitis relapses. Then, the diagnosis should be confirmed by a provocation test.
Whenever environmental allergies are implicated, and other body areas are affected, allergen-specific immunotherapy or symptomatic therapies, such as oclacitinib, lokivetmab or ciclosporin, might be discussed with owners for long-term management.
Generally, these therapies are associated with topical proactive treatment based on the use of topical steroids (hydrocortisone aceponate) applied twice a week in the ear canals. If seborrhoeic disorders are identified, ceruminolytic or ceruminosolvent ear cleaners should be used as a part of the treatment, and usually protracted as maintenance therapy.
To manage otitis in the long term, predisposing factors also should be identified and possibly avoided. Drying ear cleanser, containing astringents (acids, isopropyl alcohol or silicon dioxide) may be used prophylactically after bathing the ear or in case of swimming dogs to decrease the risk of maceration of the ear. Hairy ear canals, conformational stenotic ear canals (in brachycephalic breeds or the Shar Pei) and dogs with pendulous ears might require periodic ear cleaning to maintain normal cerumen accumulation.
Clinicians must be able to identify factors and causes involved in any case of otitis, and each of them should be addressed to obtain resolution of the infection and to reduce the risk of relapse. The use of the PPSP classification is a helpful tool in the diagnosis and management of ear disease.
In some cases, primary causes (such as atopic dermatitis), predisposing factors (conformation of the ear canal) and perpetuating factors (mineralisation of the cartilage) cannot be resolved.
In these cases, maintenance therapy is necessary, after having treated secondary infection, to prevent relapses. These “proactive” therapies might include topical steroids and/or ear cleanser (ceruminolitic/solvent/antiseptics) to enhance cerumen elimination and control microorganism overgrowth.