7 Mar 2016
Rebecca Robinson looks at ways in which pain can be assessed in companion animals using the variety of available scales (part 2 of 2).
Rebecca Robinson
Job Title
Figure 1b. Behavioural indicators are an important aspect of pain assessment, but one must be aware of the normal behaviour for species. This cat looks relaxed with its feet curled under the body and the head up. The cat looks alert and the eyes are held wide open.
A shift has been made in the attitudes towards animal pain. It is accepted animals feel pain, so there is a requirement for analgesia provision for livestock, companion and laboratory animals undergoing painful procedures.

Working within the veterinary profession, we have a moral obligation to ensure animals under our care receive appropriate analgesia. Additionally, untreated pain can result in significant delays in a return to normality with multiple physiological effects.
Management of acute, postoperative pain in companion animals was discussed in VT46.07. However, to successfully manage pain in non-verbal species, confidence in assessment is required, in terms of its absolute presence or absence and its severity. This allows an appropriate level of analgesia to be promptly administered and the required dosing frequency to be judged.
Using standardised pain scales allows a repeatable measure that is consistent between observers. Additionally, if the pain score is recorded over time, it allows an objective evaluation of a patient’s response to management.
Pain is considered to be a subjective experience; therefore, what might be painful for one individual might not be for another.
In verbal humans this problem is overcome by asking the individual to self-report. This becomes difficult when dealing with non-verbal beings, including neonatal humans or veterinary species. It falls to the carer to recognise and interpret signs of pain, which requires a certain level of skill and knowledge.
Table 1 illustrates the numerous physiological changes associated with pain. However, these changes are not specific to pain, so we cannot rely solely on such variables.
In a laboratory setting it is possible to use neurophysiological techniques (Murrell and Johnson, 2006) and measurement of plasma hormone concentrations (such as cortisol or acute phase proteins), with varying degrees of success – depending on the method employed, type of pain and species.
In clinical practice, pain assessment primarily involves recognition of behavioural alterations. This includes loss of normal behaviours and development of new ones (Table 2). It is, therefore, critical any assessor is aware of normal behaviour for the specific species (Figure 1). This is particularly important when assessing prey species, such as rodents that do not often show overt signs associated with pain, unlike the vocalisation or aggression by dogs.
Numerous factors may contribute to our poor pain recognition in these species, including how long humans have co-evolved with the species and whether overt signs of pain are likely to increase assistance from social group members or the risk of predation.


Pain assessment in non-verbal species can be complicated by external factors. The presence of environmental or situational stressors can modulate the patient’s response to pain. Administration of sedative drugs as part of a perianaesthetic protocol may mask behavioural changes associated with pain. In humans, the pain response can be amplified by anxiety, causing hyperalgesia (Colloca and Benedetti, 2007).
A similar scenario may possibly occur in veterinary species. Observer-specific factors, including age, gender, clinical experience, previous personal experience and time since graduation, can influence the overall pain assessment. For example, when laboratory mice are assessed by male as opposed to female observers, the male scent causes a stress response, resulting in stress-induced analgesia and fewer pain-induced behavioural changes (Sorge et al, 2014). Such phenomena will ultimately influence both the type and frequency of analgesia provision.
A number of different pain scales have been developed for use, most adapted from those for human medicine. A key difference between human and veterinary pain scales is in veterinary medicine all are based on observer interpretation of the intensity of the animal’s pain.
For maximal patient benefit, it is crucial only one pain scale is used throughout treatment. This allows assessment of the patient’s response to analgesic therapy and can guide future treatment. Changing between types of pain scales for individual patients is not advised, as the variation will prevent temporal comparison.
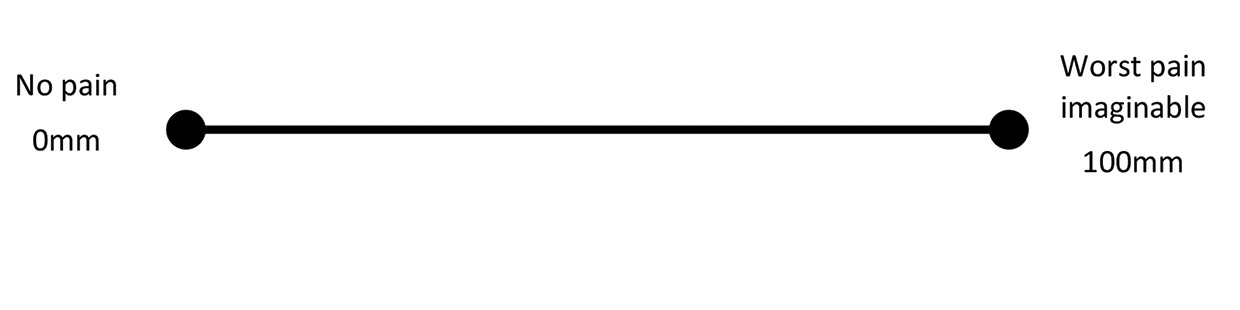
A visual analogue scale (VAS) consists of a horizontal line, normally 100mm in length. The zero end of the scale represents no pain while 100mm represents the worst pain imaginable (Figure 2). The observer marks this line corresponding to their perception of the animal’s pain. This can be quantified by measuring the distance in millimetres from zero.
Arbitrary cut-off values can be set for determining analgesia administration. Studies in human medicine suggest values lower than 35mm are consistent with mild pain, while above this value pain becomes progressively more severe (Boonstra et al, 2014). Regular, repeated assessment and recording of values allows response to analgesia to be determined.

Although simplistic and rapid to use, some degree of training is required for use, as observers need to be familiar with pain behaviours.
When used repeatedly by the same observer, VAS shows good reproducibility. However, if multiple people are involved in pain assessment there is significant interobserver variability (Holton et al, 1998), reducing their usefulness and having implications for analgesia provision in clinical settings.
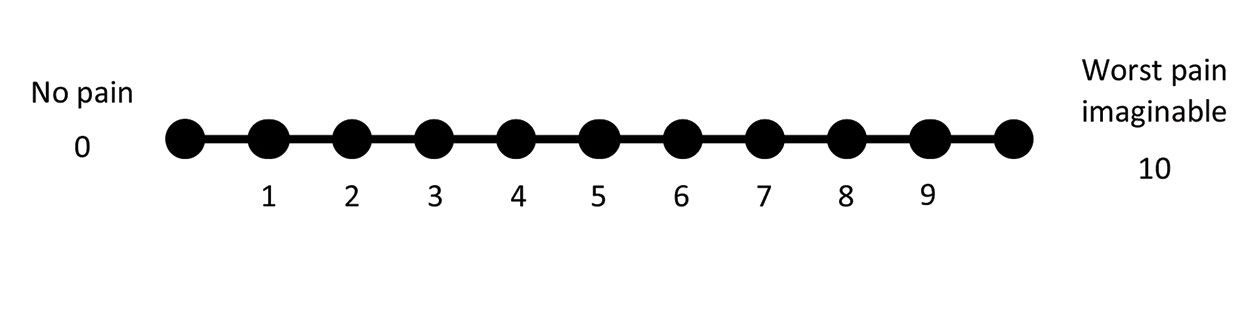
Numerical rating scales (NRS) are comparable to VAS, with similar caveats, although the scale is drawn with discrete numbers, from zero to 10, on the illustrated line (Figure 1).
As with a VAS scale, zero represents no pain and 10 represents the worst pain imaginable. Such a system may have a reduced sensitivity compared to VAS, as only whole integers are used.
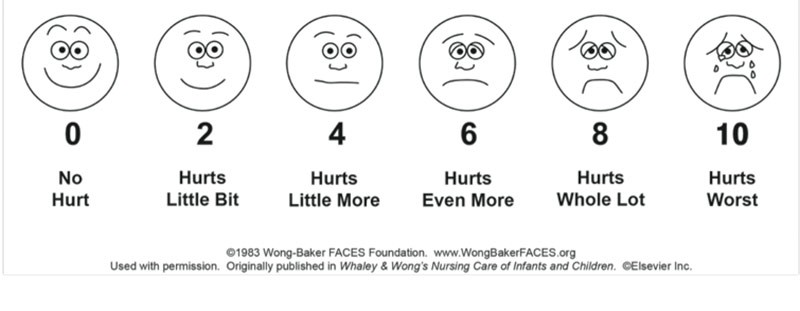
Simple description scales (SDS) have many parallels to NRS, the difference being that descriptors, rather than numbers, are used. Such descriptors may be linked to a number to convert the result to a pain score.
A widely used example in human medicine for ages three and older is the Wong-Baker FACES pain rating scale (Figure 3). The diagrammatic and descriptive representation makes it easier to understand and self-report.
Similar scales have been adapted for veterinary patients, including those produced by Colorado State University, using multiple SDS to assess acute pain in cats, dogs and horses (Colorado State University, 2006b; Colorado State University, 2007).
Dynamic interactive visual analogue scale (DIVAS) is an expanded version of the VAS. It uses the same principle of marking the perceived pain level along a 100mm line. However, DIVAS also relies on the handler interacting with the patient and gently palpating surgical wounds to provide a complete score.
VAS and NRS are considered unidimensional, as they only assess pain intensity. However, as Tables 1 and 2 show, pain affects an animal in multiple ways; therefore, multidimensional composite scales have been developed to incorporate such factors, assessing not only the physical pain intensity, but also emotional effects. Such scales often weigh behaviours and variables differently, which may help to minimise the interobserver variability seen with more basic scales. Some multidimensional composite pain scales take account of both physiological and behavioural aspects while some focus primarily on behavioural changes, usually with and without handler interaction. As with other pain scales, these rely on user experience of normal behaviour for the particular species.
The short form of the Glasgow composite measure pain scale for canine acute pain is probably the best known multidimensional pain scale. This was preceded by the University of Melbourne’s pain scale (Firth and Haldane, 1999).
There is a growing amount of research and evidence assessing how facial expressions change when an animal is in pain. This has been a well-known method of pain assessment in rats and mice in laboratory settings for many years, with the rat grimace scale and mouse grimace scale including assessment of the tightening of the orbital area, flattening of the nose and cheek, and changes in the ear and whisker position (Sotocinal et al, 2011; Matsumiya et al, 2012; Oliver et al, 2014).
Research is being performed to develop similar methods for species such as horses (Dalla Costa et al, 2014; Gleerup et al, 2015), rabbits (Keating et al, 2012) and cats (Holden et al, 2014).

Pain scales can either be non-validated or validated. The process of validation involves extensive testing of the pain scale to ensure it is reliable, giving expected results, including those across different patients and users (Brondani et al, 2013).
The process of validation assesses three aspects (Brondani et al, 2011; Table 3). Validating veterinary pain scales can be difficult, particularly for content validity (by relying on what has deemed to be important by experts) and criterion validity (a lack of “gold standard” methods of assessing pain).
In most cases, particular pain scales have been validated only for specific species and, in some instances, only for certain conditions or scenarios. Using a validated pain scale provides more consistent and accurate results, allowing easier comparison between subjects and clinical studies.
The pathophysiology of acute and chronic pain differs greatly. Acute pain is generally caused by injury and often serves a protective or biological purpose. It is usually self-limiting and associated with the timescale of normal healing. Chronic pain, however, is often considered a disease state in its own right, doesn’t serve any biological purpose and has no recognisable end point (Grichnik and Ferrante, 1991).
Both the nature of the two pain states and their behavioural indicators are different. Therefore, pain scales designed for acute or chronic pain are not interchangeable. Acute pain scales are often designed for use by veterinary personnel in a hospital environment, as this is where acute pain is most likely to be experienced. Although it is always beneficial to know the pain-free behaviour of the animal, it is possible for a naïve observer/handler who has knowledge of the general species’ behaviour to use an acute pain scale to judge the level of pain.
In contrast, behavioural changes associated with chronic pain can often be subtle and gradual in onset. As a result, such alterations can only be recognised by someone who is very familiar with the animal, usually the owner (Mathews et al, 2014). However, sometimes owners are unaware subtle changes may be associated with pain and often it is only highlighted when there is an improvement in patient demeanour during an analgesia trial.
Chronic pain scales revolve around quality of life questionnaires and functional assessment of the animal. Factors considered often include:

Patients with pain caused by ocular conditions are particularly challenging to assess. Clinical signs, such as serous ocular discharge and photosensitivity, may be associated with the underlying condition, but not necessarily pain. Conversely, other clinical signs, such as blepharospasm, are often indicative of acute ocular pain (Figure 4).
Assessment can become more difficult with ocular conditions likely to cause chronic pain, such as glaucoma. None of the veterinary acute pain scales are specific to ocular pain. However, a number of publications have used non-validated pain scales to assess ocular pain (Myrna et al, 2010; Clark et al, 2011).
A limited number of validated pain scales are available for companion animal use and may be for use in specific scenarios.
Short form of the Glasgow composite measure pain scale (Morton et al, 2005). Validated for assessment of acute pain associated with multiple conditions in dogs through a questionnaire completed by veterinary personnel.
All three have been validated for chronic pain associated with osteoarthritis through the use of owner questionnaires. The HCPI also uses a questionnaire completed by the veterinary surgeon.
Assessing pain in veterinary species can be challenging. Pre-existing knowledge of normal species-specific behaviour is essential. Pain scales enable a more objective assessment of pain and allow serial assessments
to be compared.
Regular, repeated assessments with the same scale are required to determine if there has been a positive response to analgesia provision and to guide further therapy. Use of appropriate pain scales can help improve animal welfare in an acute, postoperative setting and animal quality of life during chronic pain states.