12 Jun 2017
Becky Robinson discusses some of the best practice techniques when performing anaesthesia on small animal patients.
Becky Robinson
Job Title
Figure 1. Aspiration should be performed before any local anaesthetic block. Here, blood is welling into the needle hub after accidental vessel puncture; the needle needs to be removed and a new one repositioned before injection.
The first recorded use of local anaesthetics in veterinary medicine was 1890, where topical cocaine aided the removal of ocular foreign bodies from cattle (Jones, 2002).
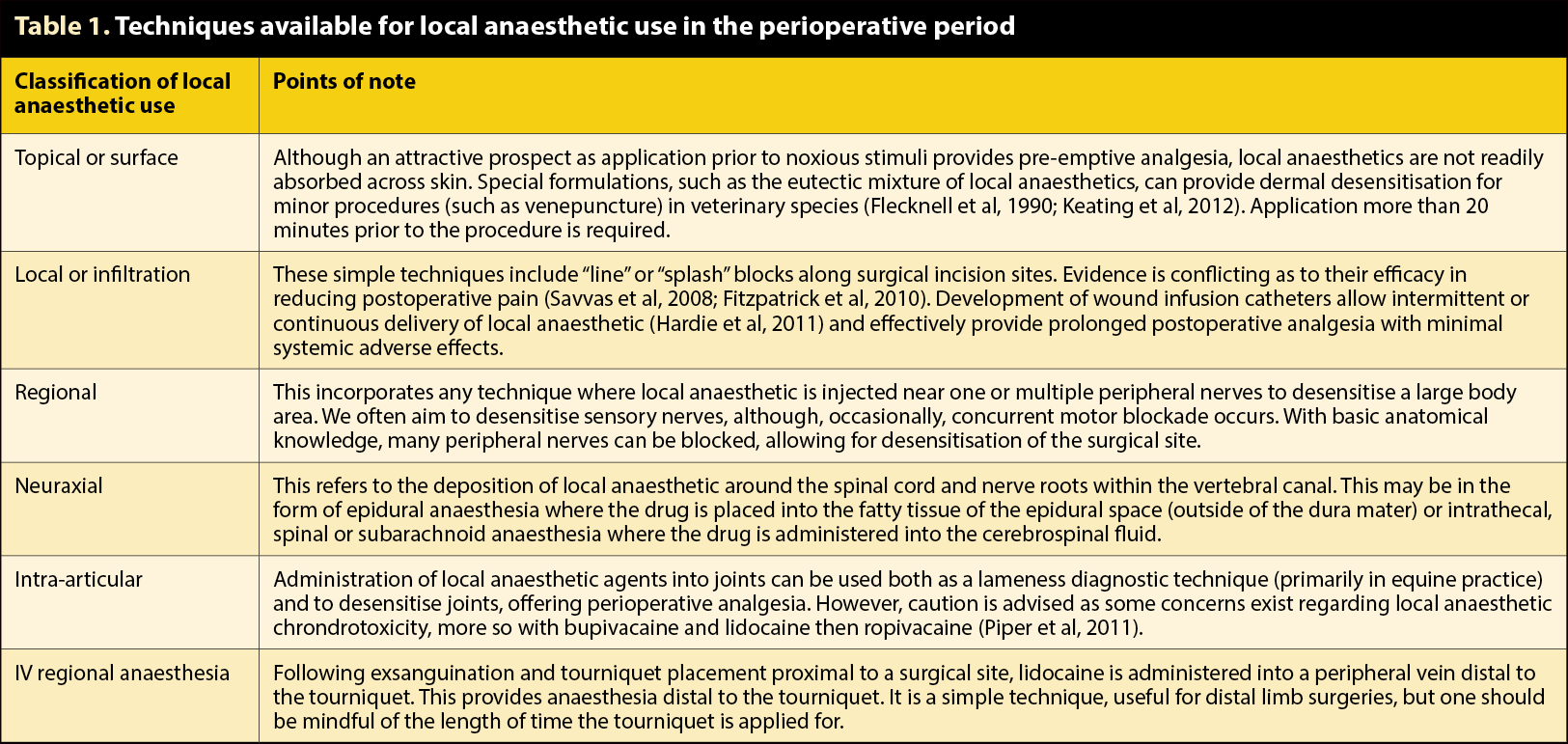
In modern veterinary medicine, use of local anaesthetics has become increasingly popular. An ever-expanding number of techniques exist (Table 1), which allow the veterinary practitioner to provide a holistic approach to perianaesthetic analgesia.
This two-part article only considers regional anaesthesia, with this part discussing the general principles behind successful techniques.
Local anaesthetic drugs are an essential part of a multimodal analgesic protocol; they are the only class of analgesic agents that can completely prevent peripheral nociceptor input and propagation of the nerve impulse. This is an important part of minimising peripheral and central sensitisation, thus reducing the chance of developing a chronic pain state.
Multiple benefits have been shown in human medicine when using local anaesthetics compared with systemic analgesia alone (AnaesthesiaUK, 2006):
Use of local anaesthetics in human medicine may prevent the need for general anaesthesia. Although the use of local anaesthesia – combined with sedative agents – is frequently used in large animal surgery, isolated reports exist in small animal surgery (Campoy et al, 2012) – often the small animal vet combines local and general anaesthetic techniques. Incorporation of a local anaesthetic technique allows for a more stable plane of general anaesthesia. It also allows for a reduction in the required concentration of inhalational agent, thus minimising associated adverse effects, such as hypotension from vasodilation and/or reduced cardiac contractility.
Local anaesthetic agents reversibly prevent nerve impulse transmission (sensory, motor or autonomic) without affecting consciousness. They achieve this though blockade of sodium channels, thus preventing sodium influx into the neurone. Drug binding sites are intracellular; local anaesthetics enter the cell through the cell membrane or open channels. This means blockade is often use-dependent.
Frequently, used nerves have more sodium channels in an open state, thus allowing increased drug passage and subsequent blocking. Practically, this means nerve stimulation (either artificially or through nociception) can decrease time to block onset.
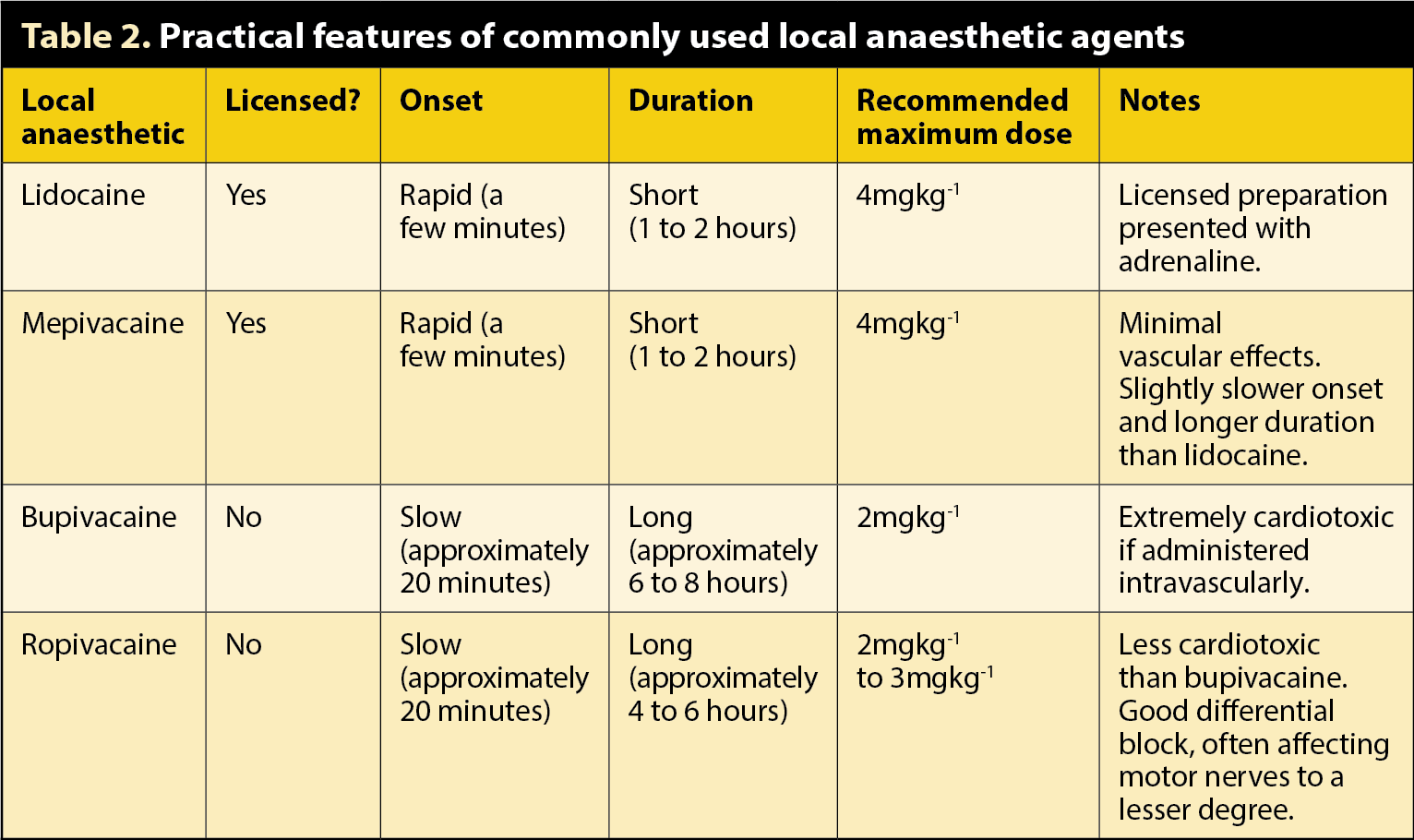
Pharmacodynamic properties, including speed of onset and duration of action, are affected by multiple physico-chemical properties, and discussion is beyond the scope of this article. A practical summary of commonly available local anaesthetics is shown in Table 2.
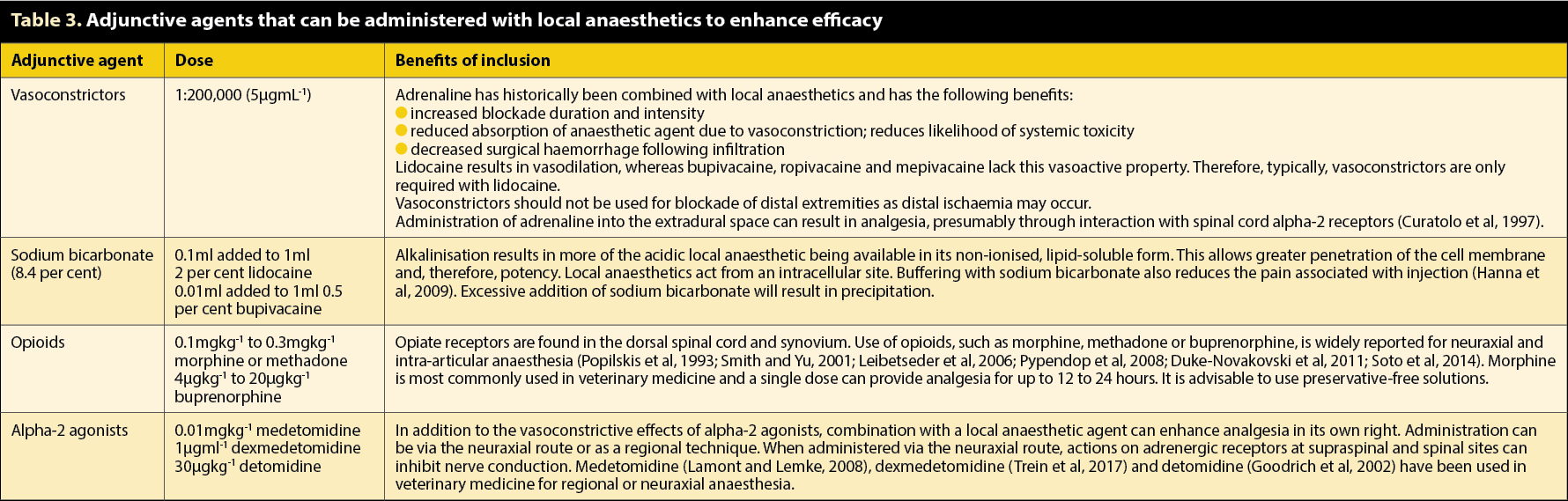
Although the obvious mainstay of regional anaesthesia is administration of local anaesthetics, adjunctive agents are occasionally included to enhance the block efficacy (Table 3).
As with any medical technique, the risk of complications exists when regional anaesthesia is performed, including the following (Jeng et al, 2010).
Signs of systemic toxicity include neurological, such as muscle tremors or seizures, and cardiovascular, including tachycardia, hypotension, arrhythmias or cardiac arrest. Neurological signs generally present prior to the cardiovascular symptoms, although in anaesthetised patients these are often masked.
Systemic toxicity most often occurs from inadvertent intravascular administration, resulting in a rapidly high plasma concentration. However, it can also arise with excessive doses used in the correct manner; despite slower absorption, toxic plasma concentrations may still be achieved.
Severity of signs depends on the drug used (bupivacaine >> ropivacaine > lidocaine), dose, rate of absorption (local tissue vascularity or addition of vasoconstrictors) and species. Cats are renowned to be more sensitive to the adverse effects of local anaesthetics compared to dogs. However, this may be due to their small size; therefore, overdose is made relatively easier.
Neurological injuries often result in neuropraxia, manifested as persistent blockade. In human medicine this is reported as increased duration of desensitisation. While difficult to identify in veterinary patients, if motor fibres are affected prolonged paralysis may be noted. Often, these injuries self-resolve, but the risk of permanent damage exists.
True allergic reactions are rare, although idiosyncratic reactions can occur. Allergic reactions are more likely after administration of ester-linked local anaesthetics due to the metabolite para-amino benzoic acid. This is mainly of concern with food-producing, large animals where procaine is the only licensed local anaesthetic.
Vascular puncture may result in systemic toxicity and such aspiration should be performed before every injection (Figure 1). Haematomas may also occur, the clinical consequences of which may vary depending on size and site; for example, the presence of a haematoma in the epidural space can be devastating.
Regional anaesthetic techniques are not always successful and failure rates in human medicine vary from 5% to 25% (AnaesthesiaUK, 2005). Failure can arise due to a variety of factors, including lack of operator experience or knowledge of anatomical landmarks; technique performed and use of aids; patient factors, including comorbidities such as obesity; and environmental factors, such as time pressures.
Veterinary studies assessing complication incidence have yet to be performed. However, reviews in human literature suggest a neurological complication rate of 0.04% after neuraxial anaesthesia and 3% after regional anaesthesia, with permanent neurological injury rare (Brull et al, 2007).
Regional anaesthesia can be performed in a “blind” manner, although a thorough knowledge of local anatomy and appropriate landmarks are essential for success. However, as discussed, block failure may occur. A number of techniques can be employed to maximise block efficacy and minimise the risk of adverse reactions.

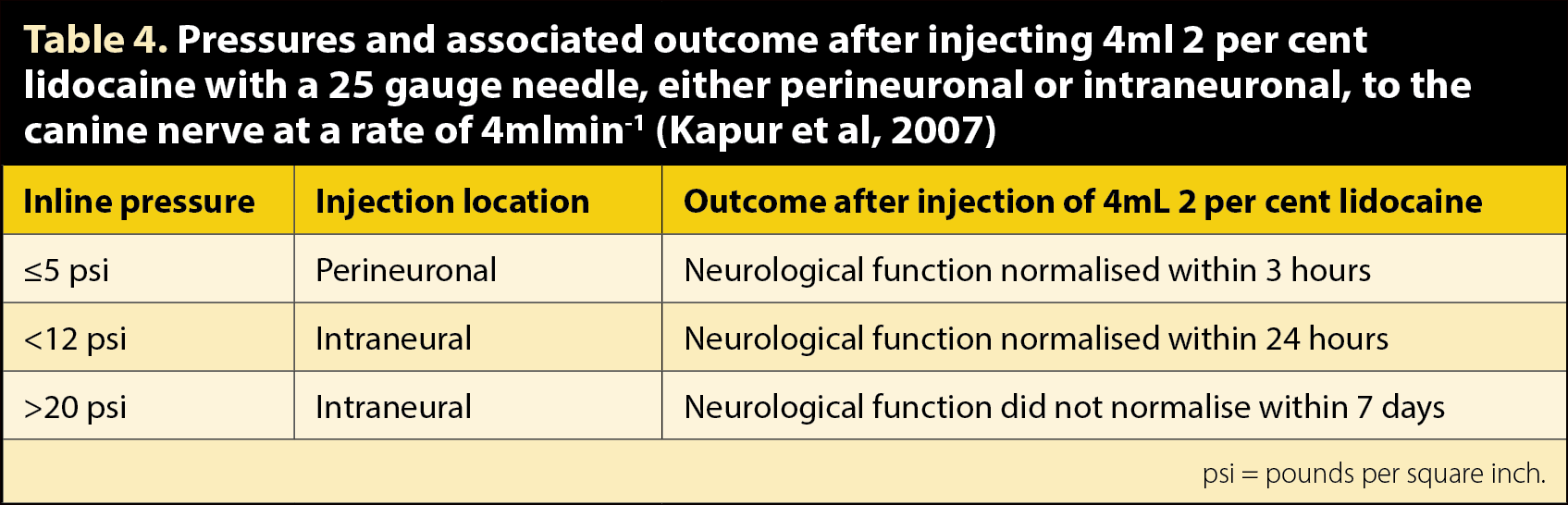
Inline pressure gauges are small, disposable devices (Figure 2) inserted between the syringe and the needle extension line. They give an objective, continuous indicator of the pressure required to inject the drugs into the tissues. This has value, as studies (Kapur et al, 2007) have shown higher injection pressures are associated with intraneural injections and, subsequently, poor neurological outcomes (Table 4).
Peripheral electro-nerve locators (Figure 3) can improve the accuracy of local anaesthetic deposition around a target nerve and successful blockade. Their use in regional anaesthesia is relatively common with multiple recognised techniques in veterinary medicine.
Nerve locators function by creating an electrical current within the tissues surrounding the target nerve. Insulated needles are used, with only a bare needle bevel, allowing for greater accuracy compared to a non-insulated needle, as the current is directed rather than being dispersed in all directions. This allows lower currents to locate the nerve (Dalrymple and Chelliah, 2006).
Providing the target nerve contains motor fibres, the electrical stimulation results in motor fibre depolarisation and specific muscle contraction. Care must be taken not to misinterpret direct muscle stimulation with muscle twitching as a result of motor fibre stimulation. The further the needle tip is from the nerve, the greater the current required to cause depolarisation. If the specific muscle contraction can be elicited at progressively lower stimulating currents it allows the user to identify he or she is close to the nerve.
Usually, the starting current for stimulation is 1mA. It is popular to aim for a muscle twitch at a current below 0.4mA, but not at below 0.2mA as this could represent intraneural needle placement (Dalrymple and Chelliah, 2006). Once a small volume of local anaesthetic is injected you would expect immediate disappearance of the twitching. This is not due to rapid onset of the local anaesthetic, merely mechanical displacement of the nerve away from the needle tip, known as the “Raj test” (Raj et al, 1980).
The use of ultrasound (Figure 3) is becoming popular in the field of regional anaesthesia. If the vet has access to an ultrasound with associated high frequency probes (9MHz to 12MHz), direct, real-time visualisation of nerve and vessel structures with good resolution can be achieved. It is also possible to view needle placement and perineural local anaesthetic spread during instillation. This offers theoretical advantages of increased likelihood of blockade success and decreased complication risk (Gray, 2006).
It does, however, require a certain degree of operator skill, which may take time to develop. Some vets combine the use of ultrasound and nerve locators in an attempt to improve accuracy.

Regardless of regional anaesthetic technique, a few general points should be adhered to. These are paramount to ensuring both good clinical efficacy and patient safety:
This article discussed the benefits of incorporating a local anaesthetic technique to help provide a multimodal approach to anaesthesia. As with any medical procedure, the chance of complications can occur, which are considered, along with methods to minimise their occurrence while improving the likelihood of a positive outcome.
Part two will highlight some of the more common regional anaesthetic techniques that can be easily integrated into an anaesthetic protocol.