3 Jul 2017
Becky Robinson looks at safe and effective techniques for applying regional anaesthesia to head, eye, thoracic and pelvic limbs.
Becky Robinson
Job Title
Figure 5. A radial, ulnar, medial and musculocutaneous block is performed using two injection sites. (5a) On the lateral aspect of the limb between the heads of the triceps and the brachialis muscle. (5b) On the medial aspect of the limb close to the site of the brachial artery.
In part one (VT47.23) of this two-part article, general principles of regional anaesthesia, including benefits, complications and aids to improving the chance of a positive outcome, were discussed.
This part will consider specific techniques for the head, eye, thoracic and pelvic limbs. Focus will be placed on the relevant anatomical knowledge and landmarks required to perform a safe and effective technique.
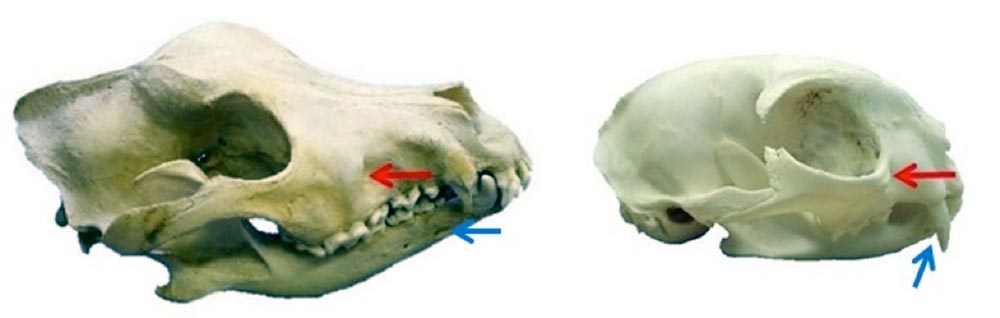


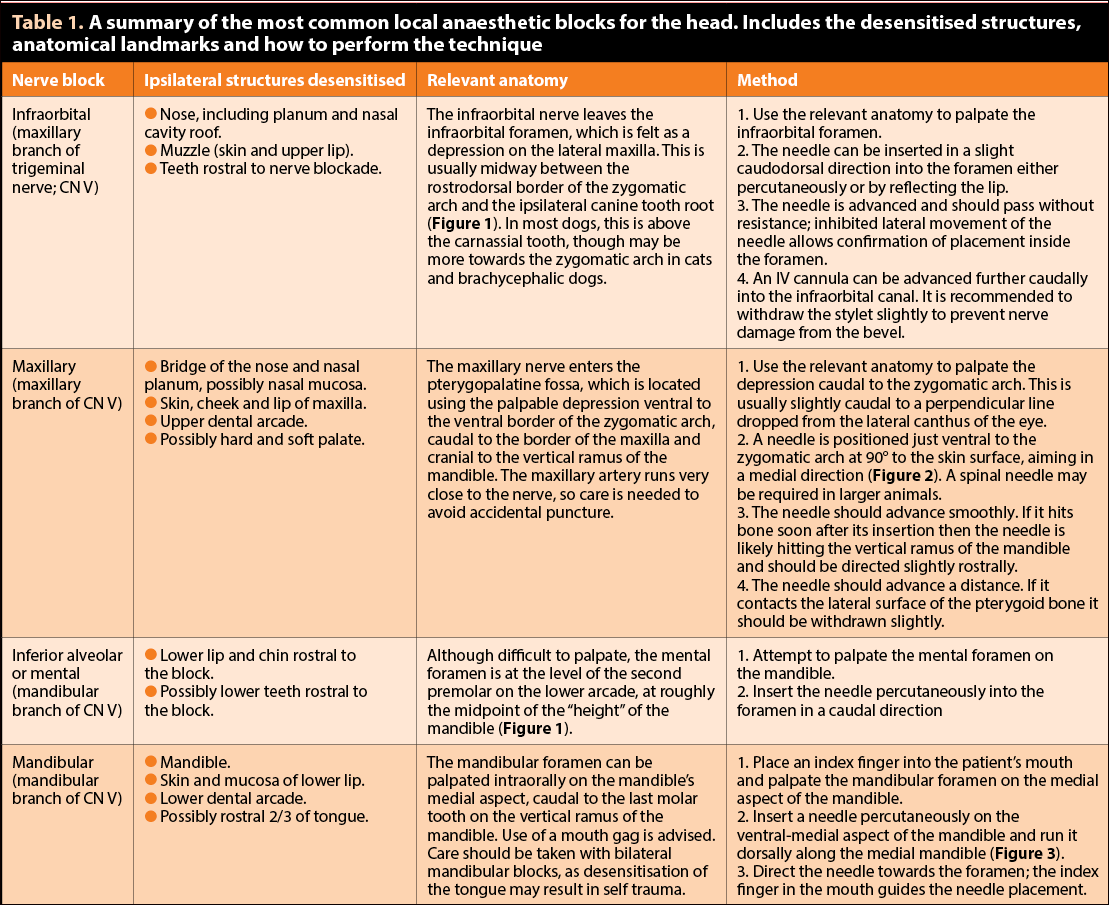
With basic anatomical knowledge, nerve blocks for the head are relatively simple and can be invaluable, particularly for dental procedures requiring extractions. The four main blocks (Table 1) useful for the veterinary practitioner are:
Absolute volumes (rather than dose) of drug are often the limiting factor, with volumes more than 3ml becoming impractical.
The retrobulbar block will desensitise the globe, eyelids and some of the upper face due to its action on cranial nerves II, III, IV, V and VI. The main indication is only for enucleation due to a number of risks associated with its use, including:
The retrobulbar block can be approached in a number of ways, the simplest being use of a curved needle (commercially available or self-curved) inserted at one point just below the dorsal orbital rim, near the lateral canthus. The needle is gently advanced behind the globe, running around the bony orbit (Figure 4). There is less risk of penetrating the optic nerve at this site compared to placement at the medial canthus. Practical volumes for retrobulbar blocks are below 2ml for cats or small dogs and below 5ml for larger dogs.

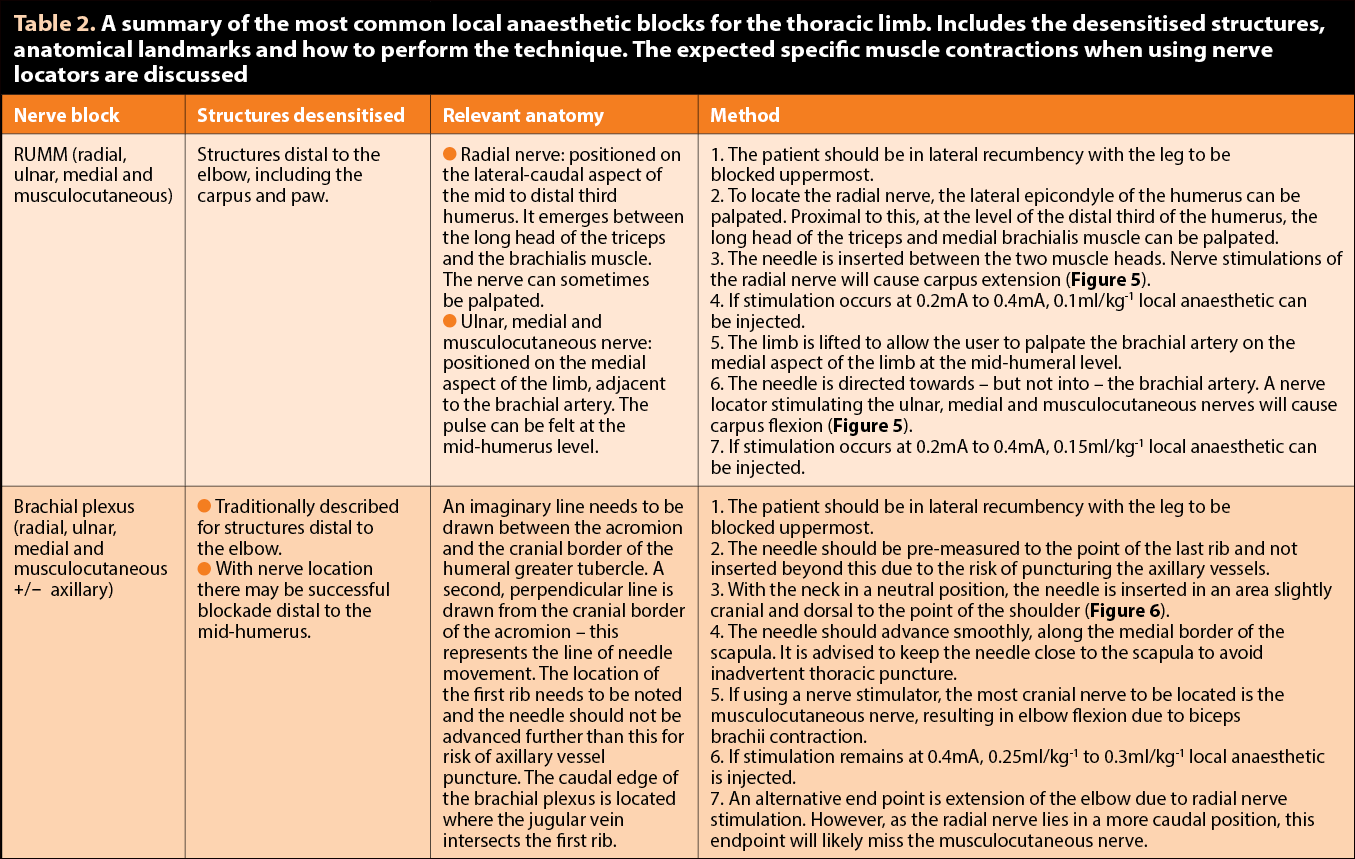
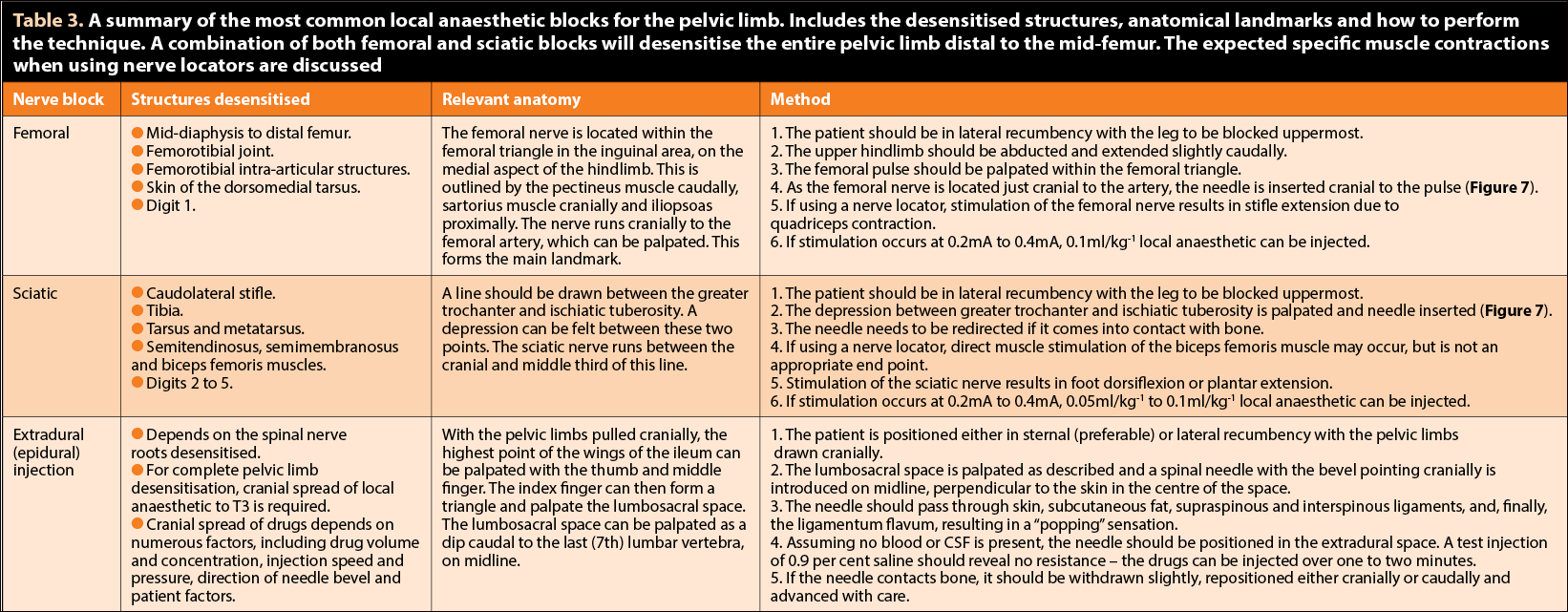
Both the thoracic and pelvic limb can benefit from regional anaesthetic techniques. The number of differing blockade methods are ever-increasing; this article focuses on those procedures considered to be the simplest, with greatest chance of success with least associated risk. Suggested thoracic limb techniques are illustrated in Table 2, with the pelvic limb in Table 3.
A ring block is slightly more advanced than infiltration; the area of interest is encircled with local anaesthetic – for example, a digit to be amputated. Vasoconstrictors should not be included if distal extremities are to be blocked, as ischaemia may result.
Neuraxial anaesthesia can also be used for blockade of the pelvic limbs, along with the perineum and abdomen. In veterinary patients, epidural (extradural) rather than spinal (intrathecal) injections are more commonly performed, usually at the lumbosacral (L7 to S1) junction.
The patient is positioned either in sternal or lateral recumbency (Figure 8). Although the procedure is briefly described in Table 3, given the greater technicality and risk associated with the procedure, readers are advised to consult additional texts for a more in-depth discussion.
Regional anaesthetic techniques enable the vet to greatly improve a patient’s analgesia.
Providing anatomical knowledge is sound, successful local anaesthetic blocks can be performed with very little equipment and cost. However, efficacy may be improved and associated risks reduced if aids, such as peripheral electro-nerve locators, are used.