1 Oct 2024
Ian Ramsey and Fergus Allerton explore how professionals can practice this, using examples.

Image © Liudmyla / Adobe Stock
The following article is structured around the concepts embedded in the BSAVA/Small Animal Medicine Society PROTECT ME1 scheme (Figure 1).
The authors will illustrate how these concepts can be put into practice, with examples and ideas for vets and nurses to discuss in their teams.
The most common misuse of antibiotics in small animal practice is the unnecessary prescription of antibiotics to animals that do not have bacterial disease.
Many clinical presentations such as diarrhoea (even when haemorrhagic), cough (even when productive), nasal discharge (even when associated with a purulent discharge) and feline cystitis (even when associated with haematuria) do not have an underlying bacterial cause. Other aetiologies such as viral infections, toxic challenge, sterile inflammatory or immune-mediated conditions are more likely.
Antibiotic therapy in these cases will be of minimal value, increasing costs to the client and potentially delaying the correct treatment. Even if secondary bacterial infection is present, antibacterial therapy may not be necessary if the underlying cause can be addressed. Furthermore, some conditions that do involve bacteria (such as kennel cough) can be managed without antibiotics.
Antibiotics should not be used as a substitute for proper surgical asepsis – they are not a safety blanket to compensate for a lack of attention to infection control.
Surgical antimicrobial prophylaxis (SAP) is an area where major reductions in antibiotic use can be achieved. No antibiotics are required for clean surgical procedures such as spays, castrates or removal of a dermal mass.
The latest PROTECT ME guidelines also recommend against the use of postoperative surgical prophylaxis (antibiotics that are continued beyond 24 hours) for all surgical procedures, even including orthopaedic procedures that involve the placement of an implant (for example, tibial plateau levelling osteotomy).
This guidance mirrors evidence-based advice from human medicine, but it is going to take time for vets to adopt these practices.
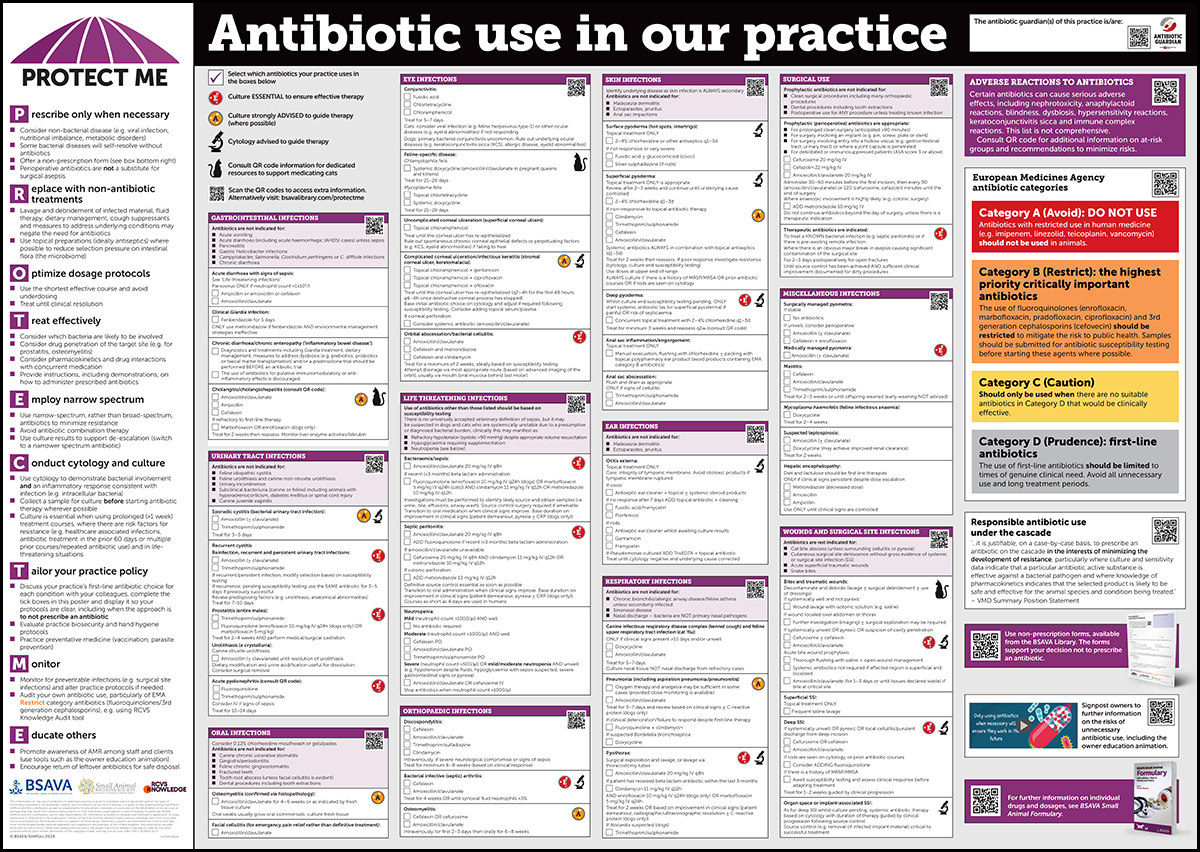
Figure 1. BSAVA and Small Animal Medicine Society PROTECT ME poster.
Do you send pets home with a course of antibiotics after a routine surgical procedure? Do you think it makes a difference? Would you consider trialling without postoperative antibiotics? If you are reading this and asking, “what’s the harm?”, and thinking, “I don’t want to be the vet with a high rate of surgical site infections”, it is worth asking yourself whether these antibiotics make any difference at all? The at-risk period is over, so what are the antibiotics doing? Furthermore, could they increase the chance that any surgical site infection that does develop may involve multi-drug resistant bacteria, making it much harder to manage?
Much great work is already underway to improve antimicrobial stewardship across the companion animal sectors; for example, part of the remit of the Responsible Use of Medicines Alliance – Companion Animal and Equine (RUMA CA&E)2 is to play a role in the reduction in the use of the highest priority-critically important antibiotics (HP-CIA).
Central to this will be to establish in which conditions HP-CIAs are most frequently prescribed.
Following stakeholder input into a roundtable event delivered by RUMA CA&E in 2022, the outputs of which were shared in its annual report3, the following clinical scenarios were identified as those to prioritise, based on where the greatest scope to improve antibiotic stewardship – particularly stewardship of HP-CIA use – was found to be present:
Rather than reaching for antibiotics, we should seek opportunities to use non-antibiotic therapies wherever possible; for example, more and more practices are stopping the use of antibiotics in acute haemorrhagic diarrhoea syndrome, with minimal impact on clinical outcomes.
More challenging to some practices is to stop using antibiotics in cat bite abscesses. However, it has been shown that cat bite abscesses can be successfully managed with lancing, drainage and effective lavage and no antibiotics; an example of this was shared in 2023 by White Lodge Veterinary Surgery, CVS.
The practice carried out a prospective audit to review the use of antibiotics, with a focus on antibiotic use in cat bite abscesses. With the introduction of checklists and in-house CPD, the team was able to treat 86 per cent of its cat bite abscess cases successfully without antibiotics and without compromising welfare4.
This audit received an Antimicrobial Stewardship Award from RCVS Knowledge in 2023 and serves as a great example of how a focused effort across a practice team can achieve positive outcomes.
A key component of good antibiotic prescribing is to use the shortest effective course, but avoid underdosing. Unfortunately, we do not know what the shortest effective course is for most conditions in veterinary medicine, and it is likely to vary from individual to individual.
Multiple trials in human medicine have found that shorter antibiotic courses are just as effective as longer ones. Is it not time to dispense with empiric treatment durations based on the number of fingers on our hands, the number of days in the week or the number of tablets in a packet?
Vets in practice are invited to contribute to ongoing research looking to establish the optimal duration of antibiotic therapy for management of sporadic cystitis in dogs (the Stop on Sunday trial). If you regularly see cystitis cases and want to help answer one of the key questions in small animal practice, contact the authors and join this study (see samsoc.org).
One practical option that may be worth trying in your practice team is to establish an initial short course for common conditions that you and your colleagues are happy with, and to give clear instructions to clients about updating the practice with a report before the course has been completed. In this way, a short window opens for re-examination if clinical remission is not achieved before the course has ended.
However, if all the reports from the owners before completion indicate that the condition has resolved, then the course can be shortened in the future and the practice policy can be refined. The concept of treatment until clinical resolution is becoming increasingly popular in both human and veterinary medicine, and will replace outdated maxims of “always complete the course”.
Route of administration can have a significant impact on the exposure of commensal organisms to antibiotics. By using topical antibiotic preparations where possible, we aim to reduce selection pressure on intestinal flora (the microbiome) and, therefore, the spread of resistance.
“Ongoing collaboration continues to be an important part of the education process, both across the profession and with clients.”
Before prescribing antibiotics, we should consider which bacteria are likely to be involved and how effectively the chosen drug will penetrate the target site.
The BSAVA PROTECT ME poster provides a starting point for which antibiotics are likely to work in specific situations, considering the ability of each medication to reach the site of infection.
When treating pyelonephritis or prostatitis, it is essential to select drugs that will achieve effective concentrations in the kidney or prostatic tissue; amoxicillin-clavulanate will not do this, so would be a poor choice for these conditions. This is the time to select a potentiated sulphonamide or a fluoroquinolone to treat effectively.
It is also important that we support owners, so they can administer antibiotics reliably. The International Cat Care website5 provides some excellent tips to help give oral tablets to cats in a stress-free manner.
Reassuring owners and finding effective tabletting techniques may be the single most likely method of effectively reducing a practice’s reliance on long-acting third-generation cephalosporins (cefovecin).
In some cases, it may be an option to provide owners with narrower spectrum antibiotic injections to administer at home.
If we can teach owners to inject insulin into cats, then we can teach some of them to inject antibiotics at home.
Broad-spectrum antibiotics (such as potentiated amoxicillin) can promote antibiotic resistance including among commensals (which, in turn, will later spread this resistance to pathogenic bacteria).
Using narrow-spectrum antibiotics limits the effects on commensal bacteria and keeps more options available for future treatment.
We can use culture results to support de-escalation (switching to a narrower spectrum antibiotic) whenever possible. Changing from a broad-spectrum to a narrow-spectrum antibiotic based on culture is good antibiotic stewardship.
Severe infections may require us to start antibiotic treatment before culture and susceptibility results are obtained. In these cases, it may be appropriate to start broad-spectrum antibiotic therapy, possibly using a combination of drugs, while awaiting results.
Combinations can be considered where activity against aerobic and anaerobic, Gram-positive and Gram-negative bacteria is required; for example, an aminoglycoside (Gram-negative spectrum) may be used alongside clindamycin (anaerobic spectrum) to treat septic peritonitis. However, that is not an excuse not to culture, but rather to highlight the value of cultures to the owners.
The costs of culturing will be more than offset by the opportunity for effective de-escalation, reducing the risk of subsequent development of multidrug resistance.
We all need to do more cytology and bacterial culture if we are to be effective antibiotic guardians6.
The best way of developing your skills in cytology is to practice it and check against the results you receive on the same samples from external laboratories. Using cytology is the quickest way of confirming bacterial involvement associated with an inflammatory response (for example, intracellular bacteria).
Samples for culture should be collected before starting antibiotic therapy wherever possible. Culture is essential when prolonged (more than one week) treatment courses are anticipated, when resistance is likely (for example, health care-associated infections) and with life-threatening infections (even if in these cases antibiotics need to be started before the results are back).
If first-line treatment fails, do not use another antibiotic without culture and susceptibility results – it is both good and economic medicine.
It should be remembered that bacterial species differ greatly in their inherent susceptibility or resistance to antibiotics. Some species have stable and predictable resistance patterns, enabling a rational antibiotic selection to be made empirically; others are more variable, and susceptibility testing is vital to guide effective antibiotic selection in these infections.

Image © Liudmyla / Adobe Stock
To achieve good antibiotic stewardship, vets need to work collaboratively within their practices.
Even if progress may appear to be slow, by building on consensus within the practice, more can be achieved over time than by one person acting independently.
A customised practice policy can guide antibiotic selection to address the bacterial infections and resistance patterns that you see, minimising inappropriate use. Completing the tick boxes in your PROTECT ME poster to highlight your practice’s first-line approach to each condition is a vital step in the practice’s antibiotic stewardship.
When developing your practice policy, it may be appropriate to consider not only which antibiotics you will prescribe, but also the diagnostic testing and adjunctive therapy that are appropriate for particular conditions.
Monitor for preventable infections in your practice (for example, surgical site infections) and alter practices if needed.
Audit your own antibiotic use – particularly of European Medicines Agency (EMA) Category B (restrict) antibiotics (such as fluoroquinolones and cefovecin).
Share this important message about antimicrobial resistance (AMR) to reduce the threat from multidrug resistant strains of bacteria and improve the health of pets and people.
Veterinarians may perceive pressure from pet owners to prescribe antibiotics; it is important to understand why owners apply this pressure.
Reasons include a lack of awareness of alternatives to antibiotics, lack of understanding of the risks of over-prescribing to them and their pet, and finally, a lack of knowledge of the adverse events associated with antibiotics. Address these issues with owners, and the pressure goes away.
In the authors’ experience, many owners who request antibiotics are more than happy not to receive antibiotics if they are provided with a well-considered reason and alternative strategies. Education of clients on the issue of AMR in animals is a clear duty of the veterinary professional.
Client pressure for antibiotics can often be lessened by providing non-antibiotic alternatives in uncomplicated viral infections or self-limiting diseases, such as cough suppressants for kennel cough, probiotics for diarrhoea and analgesia for cystitis. Several resources are now available to help educate pet owners on the importance of preventive measures and hygiene in the control of infectious disease; for example, non-prescription forms7 can be used to support your decision not to prescribe antibiotic therapy.
This simple tool has been shown to be effective in human medicine to reduce prescription rates with no negative impact on patient outcome.
Ongoing collaboration continues to be an important part of the education process, both across the profession and with clients. Campaigns such as the Veterinary Antibiotic Amnesty8 led by RUMA CA&E, which takes place annually every November, focuses hearts and minds on the important issue of AMR.
The aim of the campaign is to encourage clients to return any unused or out-of-date antibiotics. This will allow correct and safe disposal of the antibiotic medications, which will avoid contamination of the environment and help prevent AMR due to inappropriate disposal. It is a perfect opportunity for practices to have AMR discussions with clients and raise awareness.
Practices can access a campaign toolkit where they will find a wide range of resources, including posters, client handouts, practice guidelines on how to run the campaign, as well as pre-written content for practice newsletters and social media channels, via the RUMA CA&E website8.