14 Dec 2020
Roser Tetas Pont DVM, MSc, DipECVO, MRCVS and Joy Ioannides BSc, BVetMed(Hons), PGDipVCP, MRCVS detail how to examine the eye in cats when looking for signs of such conditions, including hypertension.

Figure 1. Gentle restraint of the feline patient for ophthalmic examination, with one hand under the cat’s chin to stabilise the head.
Many systemic diseases may result in ocular clinical signs. A complete ophthalmic examination can provide important information when investigating systemic diseases, and can aid in reaching a diagnosis. This article describes ocular lesions, which may be seen in some of these systemic diseases.
A common disease in which ophthalmological assessment in cats is important is systemic hypertension. Early diagnosis of systemic hypertension using blood pressure measurement and ophthalmic examination can help in early detection of systemic hypertension, and potentially avoid catastrophic target organ damage such as blindness.
Many systemic diseases can result in ocular clinical signs, and in some cases may present initially as ocular problems.
Ocular examination can provide important information when investigating systemic diseases, and can aid in reaching a diagnosis. Systemic diseases in cats that may have ocular manifestations are listed in Panel 1.
Ophthalmic examination is a cheap and useful diagnostic tool requiring minimal equipment that is widely available to the general practitioner. Ophthalmic examination should be performed in a quiet, calm environment to optimise patient cooperation – ideally in a room in which the lights can be dimmed.
An assistant or the owner should gently restrain the cat with one hand under the cat’s chin to stabilise the head (Figure 1). In all cases, the globe and the ocular adnexa should be examined in both eyes.
The handheld direct ophthalmoscope can be used to examine the whole eye systematically, using a high light intensity to test the pupillary light reflex and dazzle reflex, and a lower light intensity for close examination of the structures of the eye and to perform retroillumination.
The examination should be performed in a systematic manner to ensure no structures are missed. The authors recommend an outside to inside approach, starting with the eyelids and moving through the eye towards the fundus. See Panel 2 for suggested steps for a complete ophthalmic examination.
The indirect ophthalmoscope is useful for visualising the fundus in a wider field of view and identifying areas of concern that can then be examined at a higher magnification with the direct ophthalmoscope.
Pupillary dilation may be necessary to visualise the entire fundus and lens, and is most commonly achieved by applying one drop of tropicamide (0.5%) to the eye. After applying tropicamide, onset of mydriasis is approximately 15 minutes in cats and maximal dilation is within one to two hours; dilation can last up to nine hours post-application (Stadtbäumer et al, 2006).
It is important to measure intraocular pressure (IOP) before using tropicamide, as it can significantly increase IOP and worsen glaucoma; therefore, it is contraindicated in cats with increased IOP (greater than 25mmHg, or a difference of IOP greater than 12mmHg between eyes; McLellan and Miller, 2011).
To view the fundus with the direct ophthalmoscope, start with a moderate light intensity by looking directly through the view hole into the patient’s eye at arm’s length and identify the fundic reflex of light shining back from the tapetal fundus. Ideally, the observer’s right eye should be used to view the patient’s right eye and vice versa.
Reduce the light intensity using the rheostat on the ophthalmoscope and move closer to the eye. It is important to visualise the entire fundus – both tapetal and non-tapetal – by moving your head and the ophthalmoscope in relation to the patient (Figure 2).
To view the fundus using indirect ophthalmoscopy, a light source should be held at the level of the temple, and aligned with the fundic reflection at arm’s length. With the other hand, hold the condensing lens approximately 3cm to 5cm in front of the patient’s eye.
The image of the fundus will appear on the condensing lens and it will appear inverted, with the top of the fundus at the bottom of the condensing lens and the left side of the fundus at the right side of the condensing lens (Figure 3).
20D and 30D lenses are most commonly available in practice – as a general rule, the higher the diopter (D) of the lens, the wider field of view, but the lower the magnification. The 20D lens is good when the pupil is dilated, but the 30D lens may be useful in patients with small pupils, such as kittens, or if mydriasis is contraindicated (such as in cases with glaucoma). If available, the 2.2 pan-retinal lens provides a wider field of view at a higher magnification (Heinrich, 2014).
Systemic hypertension is relatively common in cats. It is most commonly seen in cats older than 12 years of age and is defined as a systolic blood pressure greater than160mmHg.
Distant “hands-off” examination: observe whether the patient bumps into obstacles, the facial symmetry, blink rate, ocular discharge and eyelid conformation
Schirmer tear test: the Schirmer tear test should be performed early in the ophthalmic examination, as shining light into the eye or applying drops may increase tear production
Menace response: take care not to touch eyelashes or cause excessive air movement, which may cause a blink
Palpebral reflex: test reflex at lateral canthus, and medial canthus, since each area is innervated by a different branch of the trigeminal nerve
Dazzle reflex: performed with bright light
Pupillary light reflex (PLR): remember, negative PLR does not necessarily indicate blindness and positive PLR may be present in blind cases
Eyelids: assess eyelid confirmation and examine eyelid margins for abnormal eyelid conformation or hairs rubbing the eye, evert the eyelids to examine the palpebral conjunctiva
Conjunctiva: examination of palpebral and bulbar conjunctiva
Cornea: using the direct ophthalmoscope, assess smoothness and transparency of the cornea and presence of lesions
Anterior chamber: observe clarity and depth
Iris and pupil: iris should be assessed for colour and irregularity, while pupils should be symmetrical, move freely and have the same size in both eyes
Lens: note position and size of any opacities. Pharmacological mydriasis may be necessary to assess the whole lens
Fundic examination: pharmacological mydriasis is usually necessary. Direct or indirect ophthalmoscopy may be used, low light intensity increases patient compliance
Fluorescein stain: flush away excess stain using sterile saline
Intraocular pressure (IOP): measurement with rebound or applanation tonometer. Normal IOP in cats is 10mmHg to 25mmHG, and the difference between eyes should be no greater than 12mmHg
The eye is a target organ for systemic hypertension and it has been suggested that 40% to 65% of hypertensive cats have evidence of ocular involvement (Elliott et al, 2001; Jepson et al, 2007; Stepien, 2011). Ophthalmic abnormalities are caused by damage to the retinal and choroidal vasculature walls, and may manifest as a variety of ocular lesions (Panel 3); often more than one of these lesions is present. Lesions are usually bilateral, although often differ in severity between the two eyes (Maggio et al, 2000).
Blindness caused by complete retinal detachment may be the first problem noticed; however, in cats presenting earlier in the disease course, more subtle ocular lesions may be noticed. Identification of abnormalities on ophthalmic examination may make it possible to diagnose cats with systemic hypertension earlier, before devastating target organ damage such as blindness occurs.
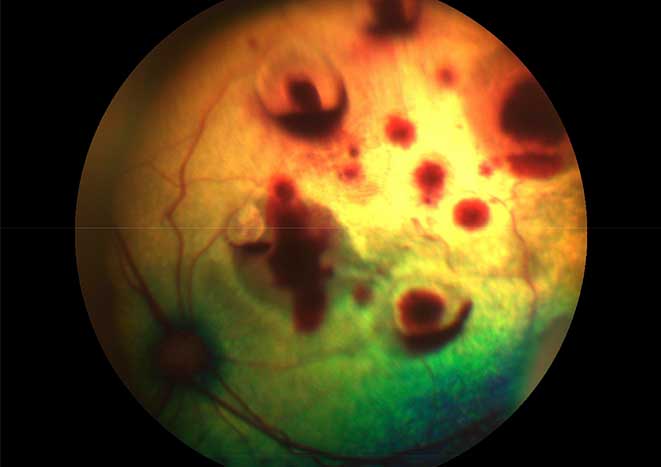
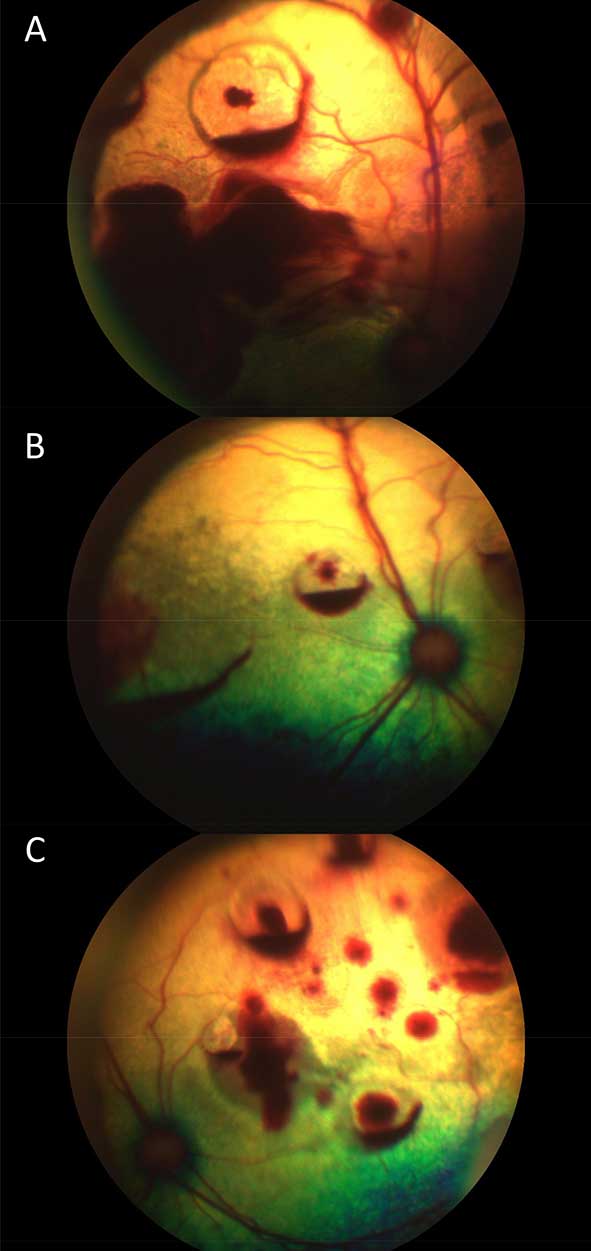
Early in the disease course, subtle changes to the retinal arterioles may be noticed; increased tortuosity and segmental narrowing of retinal arterioles. Retinal haemorrhage and retinal oedema are seen as variable sized red (haemorrhage; Figure 4) or grey (oedema) hyporeflective patches on the tapetum and are usually multifocal, but may be generalised.
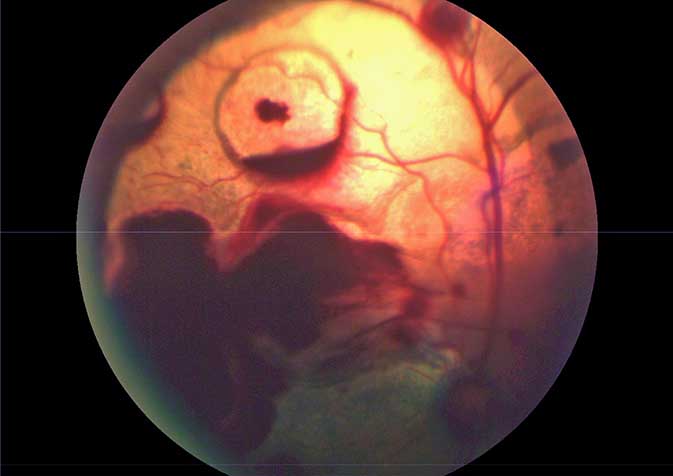
Subretinal oedema arising from damaged choroidal vessels is also relatively common, and is seen as single or multiple retinal detachments. Hyphaema (blood in the anterior chamber) may be associated with retinal detachment (Figure 5).
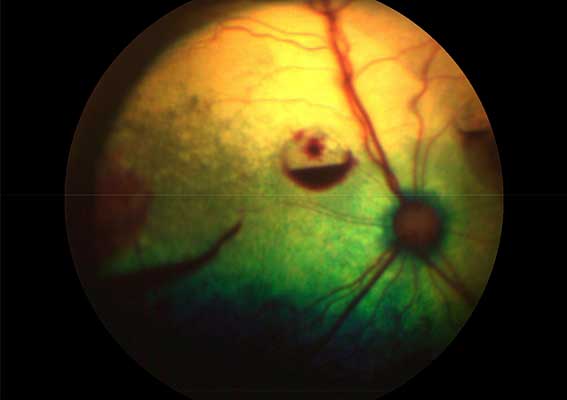
Ocular ultrasonography may be required for the diagnosis of a retinal detachment if direct examination of the ocular fundus is not possible (Figure 6). Retinal detachment can progress to retinal degeneration (tapetal hyper-reflectivity) due to lack of blood supply. Optic nerve head oedema is seen in cases of severe hypertension; the optic nerve head appears swollen with a hazy outline (Crispin and Mould, 2001).
Ocular lesions have been shown to improve with appropriate treatment achieving systolic blood pressure less than 160mmHg. Vision impairments may not improve; however, cats may adapt to cope with reduced vision. If hypertension is noticed before complete blindness has occurred, prompt treatment can preserve vision by slowing the progress of target organ damage (Maggio et al, 2000; Crispin and Mould, 2001; Jepson et al, 2007).
Systemic hypertension is most commonly diagnosed in older cats, and in cats with chronic kidney disease, hyperthyroidism and other systemic diseases (Jepson et al, 2007); therefore, regular ophthalmic examination and blood pressure measurement in cats older than 12 years of age and those with known predisposing diseases is recommended to enable early detection.
Anaemic cats may exhibit pale retinal vasculature. Retinal haemorrhage may also be present, thought to be associated with increased fragility of retinal vasculature (Gould and Carter, 2014).
Icterus can be seen as yellow discolouration of the conjunctival mucous membranes and sclera (Figure 7), typically when serum bilirubin concentration is increased greater than fivefold to tenfold above the normal reference range. Icterus may also cause colour changes in the iris; blue irides may appear green (Sherding, 2000).
Hyperviscosity can be associated with a number of disease processes, including polycythaemia and hyperglobulinaemia secondary to multiple myeloma, chronic inflammation or infection.
Ocular manifestations include increased tortuosity of retinal vasculature, retinal haemorrhage and, in severe cases, retinal detachment with or without intraocular haemorrhage (Gould and Carter, 2014).
Elevated blood cholesterol and/or triglyceride levels can cause lipid deposition in various locations in the eye; retinal vasculature, anterior chamber and/or cornea (Gould and Carter, 2014).
Thrombocyte deficiency can cause ocular or periocular haemorrhage, usually occurring when platelet count is below 50,000cells/µl (Aroch et al, 2013).
Feline dysautonomia is a disease characterised by autonomic nervous system dysfunction, along with systemic signs including malaise, dysphagia, vomiting or regurgitation, bradycardia, urinary bladder distension and constipation. Ocular signs reported reflect loss of autonomic input, and include dilated, unresponsive pupils; decreased tear production; and protruding third eyelid (Cullen and Webb, 2013).
Along with causing upper respiratory disease, feline herpesvirus (FHV-1) is also a common cause of conjunctivitis and keratitis. Keratitis can be unilateral or bilateral and is classically seen as corneal ulceration, with a characteristic “dendritic” appearance (Figure 8). It is also associated with keratoconjunctivitis sicca and corneal sequestrum (Andrew, 2001; Lim et al, 2009).
FHV-1-associated conjunctivitis is usually bilateral, manifesting as hyperaemia with serous to mucopurulent discharge; conjunctival swelling may occur, but usually to a lesser extent than with bacterial conjunctivitis (Andrew, 2001). Infection of kittens in utero can result in kittens born with adhesions between the eyelids or between conjunctiva and cornea.
Chlamydophila felis causes acute and chronic conjunctivitis, and may be associated with signs of upper respiratory tract disease. C felis can be transmitted from cat to cat via direct contact. Cats infected with C felis may also have co-infections with other bacteria or viruses.
FIP (caused by feline coronavirus with mutation) can present in effusive, non-effusive or mixed form. Ocular signs are more common in non-effusive FIP. Anterior uveitis is the most common ocular sign (Figure 9), and is often seen with keratic precipitates and a fibrinous exudate in the anterior chamber; chorioretinitis with retinal vascular changes may also be seen.
Ocular signs are usually bilateral, but severity often differs between eyes (Gould and Carter, 2014; Cullen and Webb, 2013).

Toxoplasma can cause uveitis and chorioretinitis. Optic neuritis has also been reported. Affected cats will usually also show systemic signs such as gastrointestinal signs, pneumonia, neurological signs, pyrexia and anorexia; however, ocular manifestation without systemic signs is possible.
Transplacental infection is possible; if a queen is infected during pregnancy, kittens may be stillborn or neonates may show ocular signs along with other systemic problems (Cullen and Webb, 2013; Davidson and English, 1998).
Diabetes mellitus is common in cats; however, in contrast to dogs, cats are resistant to forming diabetic cataracts.
Reports have existed of systemic neoplasia with ocular metastases including lymphosarcoma, adenocarcinoma, osteosarcoma and plasmacytoma (Figure 10). Neoplasia affecting the middle cranial fossa disease can also present with ocular signs, such as mydriasis (Figure 11; Hamzianpour et al, 2018).
Taurine insufficiency is becoming rare with the addition of taurine to commercial cat food, but may still be seen in cats fed vegetarian, vegan or home-cooked, non-complete diets. It manifests as a focal central area of retinal degeneration affecting the area centralis, initially with grey discolouration, progressing to hyper‑reflectivity that, over time, progresses to affect the entire retina.
Early changes are partially reversible; however, continued degeneration results in irreversible blindness. Taurine deficiency is also associated with cardiomyopathy; therefore, if retinopathy suggestive of taurine deficiency is identified, cardiac evaluation is recommended (McLellan and Narfstrom, 2014).
In conclusion, many systemic diseases in cats have ocular manifestations for which an ophthalmological examination can aid diagnosis. Ophthalmic examination should be a part of examination of all cats with suspected systemic illness and should be performed routinely in older felids to facilitate early detection of systemic disease.