20 Jun 2016
Karen Perry in the second of a two-part article, explains how results from research into drug treatments for osteoarthritis-related pain in dogs looks encouraging.
Karen Perry
Job Title
Figure 1. Mediolateral, caudocranial and two oblique views of the talocrural joint of a three-year-old Newfoundland with severe osteoarthritis secondary to an osteochondritis dissecans lesion affecting the medial trochlear ridge of the talus. This dog did not respond satisfactorily to conventional medical or surgical management.
Osteoarthritis (OA) is a common problem in dogs and management can be challenging. NSAIDs are an integral part of OA management, but concerns exist regarding their side effects. Despite multimodal management with NSAIDs, additional analgesics, nutraceuticals, exercise modification, physical therapy and weight management, some dogs do not achieve a pain-free state, and it is recognised a large unmet need remains for further options in the struggle against OA-related discomfort. Research is ongoing in this field searching for additional pharmacologic options to improve patient response rates and reduce associated side effects. Encouraging results have been reported for grapiprant, diacerein and anti-nerve growth factor antibody, which may become valid choices in the battle against OA-related pain in the future.
As discussed in part one (VT46.16), despite the available therapeutics, many dogs continue to suffer chronic pain and disability associated with osteoarthritis (OA), and a large unmet need for alternative treatments remains (Figure 1).

For many years, NSAIDs have been the mainstay of medical treatment for OA, which act by inhibiting the cyclooxygenase (COX) enzymes needed to produce prostaglandins and thromboxanes. The goal of COX inhibition is to reduce the amount of inflammatory mediators, such as prostaglandin E2 (PGE2), which produce pain and inflammation by dilating blood vessels, potentiating chemical mediators of inflammation and hypersensitising central and peripheral nociceptors (Innes et al, 2010; Curry et al, 2005; Lin et al, 2006). However, NSAIDs used to treat OA in dogs inhibit the production of other important prostaglandins too.
Newer drugs primarily involved with COX-2 inhibition are more selective than older drugs for inhibiting the formation of prostaglandins induced by pain, inflammation and fever (Curry et al, 2005; Bergh and Budsberg, 2005). However, COX-2 is also constitutively produced in other tissues, such as the brain and kidney, where it converts arachidonic acid to prostaglandins – both of which play an important role in organ function (Bergh and Budsberg, 2005).
While these NSAIDs are considered to be effective treatments for the pain associated with OA, these COX-inhibiting drugs also carry the potential for adverse effects, including gastrointestinal ulceration and perforation and renal insufficiency (Lascelles et al, 2005; Monteiro-Steagall et al, 2013). Many dogs do not tolerate these drugs, and alternative options for pain relief are required.
Advances are being made in pursuit of more targeted pharmacologic approaches and drugs with different modes of action. These aim to increase the proportion of dogs suffering with OA – which achieve a pain-free state – with fewer, less severe associated side effects.
A more targeted approach for OA treatment in comparison with the commonly used NSAIDs would, ideally, be to block only the prostaglandin pathway primarily responsible for the pain and inflammation of OA, without impacting the production and activity of other homeostatic prostanoids produced by the COX enzymes (Rausch-Derra et al, 2015). A treatment that targets only the appr opriate molecular pathway has been a long sought after goal of OA management (Benson et al, 2011).
Prostanoids are metabolites of arachidonic acid that mediate pain and inflammation. They have been the target of medicinal therapies for centuries (Appelboom, 2002; Curry et al, 2005). However, until recently, preparations aimed at inhibiting the action of prostanoids have, with varying degrees of prostanoid specificity, prevented their production, which impacts both pathologic and homeostatic activity (Curry et al, 2005; KuKanich et al, 2012). Prostanoids are responsible for a wide range of homeostatic functions, including regulation of renal haemodynamics and ion transport, gastrointestinal cytoprotection and motility, vascular and bronchial smooth muscle activity, immune function and platelet aggregation (Woodward et al, 2011; KuKanich et al, 2012).
After the identification of prostanoid receptors in the 1990s, significant research ensued into methods of targeting each receptor with synthetic agonists and antagonists (Woodward et al, 2011). In 2013, the World Health Organization (WHO) defined a newly recognised class of drugs that act as prostanoid receptor antagonists (PRAs) as the piprant class (WHO, 2013).
PGE2 is the most abundant prostaglandin in synovia and plays a pivotal role in the development of joint inflammation and pain (Clark et al, 2008). PGE2 has four receptors (EP1, EP2, EP3 and EP4), through which it exerts its effects. Of the four receptors, EP4 has been identified as the primary mediator of the PGE2-elicited sensitisation of sensory neurons and PGE2-elicited inflammation (Southall and Vasko, 2001; McCoy et al, 2002; Lin et al, 2006; Nakao et al, 2007; Clark et al, 2008; Chen et al, 2010; Boyd et al, 2011), blocking the EP4 receptor results in substantial pain reduction (Lin et al, 2006; Nakao et al, 2007). The EP4 receptor has also been identified as being specifically involved in the pain and inflammation associated with experimentally induced arthritis in rodents (Clark et al, 2008).
Grapiprant is a new analgesic and anti-inflammatory drug in the piprant class (WHO, 2013) – a potent and highly selective antagonist of the PGE2 EP4 receptor (Nakao et al, 2007). The anti-inflammatory effects of EP4 receptor antagonists have been investigated in animal models of inflammation. In a study by Clark et al (2008), rats with an adjuvant-induced arthritis showed reduced joint inflammation when treated with an EP4 PRA when compared to those treated using EP1 or EP3 PRAs. This reduction in inflammation was comparable to that seen in mice treated with a COX-2 inhibitor. A study by Murase et al (2008) reported similar findings in a model of chronic inflammatory pain in rats, with results being similar to those achieved using rofecoxib (a COX-2 inhibitor).
Chen et al (2010) used a mouse model of inflammatory arthritis to show an EP4 PRA suppressed inflammatory cytokine production, suppressed disease and slowed disease progression. These studies support the anti-inflammatory role of EP4 receptor antagonism in rodents and demonstrate they may reduce inflammation as effectively as COX-2 inhibitors. Grapiprant specifically has been shown to reduce acute and chronic pain and inflammation in rat models of arthritis (Nakao et al, 2007; RaQualia et al, 2007a,b). Grapriprant exhibited dose-dependent and significant anti-inflammatory effects on paw swelling, inflammatory biomarkers in the serum and inflammatory markers in the synovium with efficacy comparable to rofecoxib and piroxicam (RaQualia, 2007b).
Not only is the EP4 receptor prominently involved in inflammation and pain, but it may also mediate central sensitisation and play a role in chronic pain (Kirkby Shaw et al, 2016). Lin et al (2006) reported in rodents the EP4 receptor is expressed by sensory neurons and the level of EP4 receptors increases following peripheral inflammation. Administration of an EP4 PRA decreased the associated pain and hypersensitivity in this study.
Grapiprant has been shown to selectively block the EP4 receptor in humans and dogs, as well as rodents (RaQualia, 2007c). Grapiprant has undergone experimental and pilot studies in laboratory and client-owned dogs. As part of the development of grapiprant for Food and Drug Administration (FDA) approval for dogs with OA, a safety study in healthy beagles was carried out. Long-term (up to nine months) daily oral administration of grapiprant was shown to be safe in healthy dogs at a dose of up to 50mg/kg (Rausch-Derra et al, 2015).
Grapiprant resulted in few minor toxic effects with only mild signs of gastrointestinal disturbance, such as occasional vomiting and soft or mucoid faeces that occasionally contained blood. No grossly apparent pathological changes were detected on postmortem examination and only one dog had histopathological changes in the form of mild regeneration of ileal mucosal epithelium (Rausch-Derra et al, 2015).
Effects on the gastrointestinal tract were mild, even at daily doses of 50mg/kg, which is about 25-fold as high as the therapeutic dose of 2mg/kg identified in efficacy studies involving client-owned dogs with OA conducted in support of FDA submission for drug approval (unpublished data).
No adverse effect was severe enough to require withdrawal from the study. The lack of toxic effects is not surprising given grapiprant targets only the PGE2 EP4 receptor without appreciable effects on the production or expression of other prostanoids.
A multi-site, masked, placebo-controlled, randomised field trial for the control of pain and inflammation associated with OA in dogs was completed, submitted to, and accepted by the FDA in support of regulatory approval (approved 20 March 2016). The efficacy and safety data regarding this new product were presented at the American Animal Hospital Association annual conference in Austin, Texas on 2 April 2016, and the new grapiprant tablets are expected to be available to vets from autumn 2016.
Studies are underway investigating the use of grapiprant in cats, but, as yet, data are not available (Kirkby Shaw et al, 2016). Once it becomes commercially available, grapiprant may offer a more targeted, and potentially better-tolerated, method of pain management in dogs with OA (Kirkby Shaw et al, 2016).
Reports have described drugs with the ability of providing symptomatic relief by targeting the underlying pathology of OA – particularly in cartilage and subchondral bone – with fewer associated side effects than NSAIDs. These agents have been classified as symptomatic slow-acting drugs for OA (SYSADOAs), which are expected to delay, stabilise or reverse the pathological changes in osteoarthritic joints, thereby limiting progression of the disease (Qvist et al, 2008). This class of drugs includes diacerein, an anthraquinone derivative (4,5-diacetyloxy-9,10-dioxoanthracene-2-carboxylic acid), which is an oral anti-inflammatory, analgesia and antipyretic agent with interleukin 1β (LI-1β) inhibitory properties developed specifically for the treatment of OA.
The contribution of pro-inflammatory cytokines to cartilage degradation in OA is well recognised (Fernandes et al, 2002; Pelletier et al, 1997), including IL-1β, which stimulates the degradation process of cartilage and suppresses cartilage matrix synthesis. Rhein, the active metabolite of diacerein, has been shown, both in vitro and in vivo, to inhibit IL-1β, as well as reducing collagenase production by chondrocytes and fibrinolytic activity in synovial fluid and stimulating the production of cartilage growth factors (Martel-Pelletier et al, 1998; Yaron et al, 1999; Felisaz et al, 1999). These findings led to suggest diacerein may be a viable therapeutic option for OA, without the side effects of NSAIDs (Fidelix et al, 2006).
A meta-analysis of controlled clinical studies with diacerein in the treatment of OA in humans investigated the evidence for its symptomatic efficacy (Rintelen et al, 2006). This provided evidence for statistically significant and clinically relevant efficacy of diacerein on improvement of pain and function in patients with OA.
The improvements in pain and function during the active treatment period were of a similar level to those experienced with NSAID treatment. In most of the trials evaluated, acetaminophen was permissible as an escape medication in both the diacerein and control groups, and this must be taken into consideration. However, while the mean intake of this rescue analgesia was similar during active treatment periods with either NSAIDs or diacerein, intake increased significantly in the NSAID groups once treatment ceased, while a similar increase in intake was not noted in the diacerein groups (Rintelen et al, 2006).
At the end of treatment, SYSADOAs are supposed to have an effect carried over (Lequesne et al, 1994). In this meta-analysis, significant evidence was found for this carried-over effect following treatment with diacerein with respect to pain and consumption of escape medication. This meta-analysis also indicated, with respect to tolerability, diacerein may have some advantages when compared to long-term treatment with NSAIDs (Rintelen et al, 2006).
Since this meta-analysis was performed, studies in humans have continued to suggest a beneficial role of diacerein in the management of OA with results similar to those obtained with NSAIDs during the active treatment phase. Bartels et al (2010) described a small reduction of pain in patients treated with diacerein during the first six months. Pavelka et al (2007) reported a statistical superiority of diacerein versus placebo in pain control and tenderness of the joint, and Singh et al (2012) reported an additive effect with diclofenac for pain and improvement of joint range of motion.
In a previous study in dogs (Smith et al, 1999), diacerein treatment significantly reduced the severity of morphologic changes in the stifle joint compared to placebo using the Societé Francaise d’Arthroscopie score. In the same study (Smith et al, 1999), the Mankin scores (a histologic scoring method of disease) were also lower for the diacerein group. A study investigating the effect of diacerein on cartilage and subchondral bone in the early stages of OA in a rabbit model indicated diacerein may be able to ameliorate the swelling and surface alterations of cartilage and may exert an anti-inflammatory effect on the synovial membrane, which may delay OA progression (Permuy et al, 2015). An anabolic effect on subchondral bone was also noted in this study.
Further studies are required to confirm or exclude diacerein as a useful component of OA treatment in dogs, but these initial findings are encouraging and this is definitely a treatment to watch out for in the future.
Targeting nerve growth factor (NGF) has emerged as a potentially useful therapeutic avenue for pain control. NGF was originally identified as a critical factor for the development and maintenance of sensory and sympathetic neurons in the developing nervous system. However, it is now clear the dependence of these neurons on NGF for survival is restricted to a brief time during development, and in the adult system NGF has an important role in pronociception through its effects on the NGF-specific tyrosine kinase receptor (TrkA; Lascelles et al, 2015; Hefti et al, 2006). In the adult, NGF is an important mediator in the sensation of various types of pain, including pain attributable to OA (Watson et al, 2008).
Given its role in nociception, various ways of preventing activation of TrkA have been explored, including removing free NGF, preventing NGF binding to TrkA, or preventing activation of TrkA (Eibl et al, 2012). Of these approaches, neutralising monoclonal antibodies (mAb) targeting NGF (“removing free NGF”) has been developed first.
Inhibition of NGF function via anti-NGF antibodies markedly reduces hyperalgesia and behavioural indicators of pain in various animal models of inflammatory arthritis (Shelton et al, 2005, Ghilardi et al, 2012). In human clinical studies, several anti-NGF mAbs have been evaluated and been shown to reduce pain and improve function in patients with OA (Balanescu et al, 2014; Tiseo et al, 2014; Sanga et al, 2013; Brown et al, 2012; Lane et al, 2010).
A canine-specific mAb against NGF (termed NV-01) has been described and reported to have high affinity and potency, a long half-life and low immunogenic potential (Gearing et al, 2013). A report by Webster et al (2014) suggested this canine-specific NGF mAb may be effective for the alleviation of signs of pain in dogs with OA for up to four weeks based on canine brief pain inventory (CBPI) scores. In this study, dogs had lower CBPI pain severity and pain interference scores at two and four weeks following IV administration of anti-NGF mAb when compared to dogs that received the placebo. The percentage decreases in these values were similar to those in CBPI scores in another study after administration of carprofen (Brown et al, 2008).
A further study (Lascelles et al, 2015) investigated the pain-alleviating and activity enhancing effects of NV-01 in dogs with degenerative joint disease-associated pain using the primary outcome measures of owner-completed clinical metrology instruments (CMIs) and actimetry data, using an accelerometer to record the spontaneous activity of each individual dog. The results of this study indicated a single IV injection of NV-01 decreased pain and improved mobility over a four-week period in dogs with degenerative joint disease-associated pain. Overall, the degree of reduction in pain over placebo across the CMIs was about 30%, which is considered a relevant improvement in human medicine (Lascelles et al, 2015).
The improvement in CMI data suggested the efficacy of a single dose of NV-01 was at least identical to that of daily NSAID administration. Mobility, as measured by accelerometry, was also significantly improved in dogs receiving NV-01 in comparison to those receiving placebo (Lascelles et al, 2015). The study indicated the improvement lasted for at least 28 days, but the duration of action remains unknown and may be longer. In human trials with several versions of anti-NGF mAbs, efficacy is generally detected within two weeks and appears to last at least eight weeks (Balanescu et al, 2014; Tiseo et al, 2014; Sanga et al, 2013; Brown et al, 2012; Lane et al, 2010; Bannwarth and Kostine, 2014).
The studies carried out in dogs thus far have been small, including only 11 (Webster et al, 2014) and 26 dogs (Lascelles et al, 2015). Neither of these studies were appropriately powered to assess the potential for side effects. In human clinical trials, two main types of side effects have been noted with anti-NGF mAbs – neurological effects and effects on progression of OA (Bannwarth and Kostine, 2014). In the study by Lascelles et al (2015), a complete neurological examination was performed on all study participants 28 days following treatment and no neurological abnormalities were detected. However, the abnormalities reported in people were peripheral sensory symptoms, primarily paraesthesia, hypoaesthesia and hyperaesthesia, and these would be difficult to detect in canine patients.
Human clinical studies of anti-NGF mAbs were halted by the FDA due to adverse events related to a rapidly progressing OA in about 1% of treated patients (Bannwarth and Kostine, 2014). While this was not noted in either study performed in dogs to date, larger studies are required to investigate this in addition to clarifying the duration of effect of this treatment. Pending larger studies, this represents a potential future addition to the arsenal in the treatment of OA.
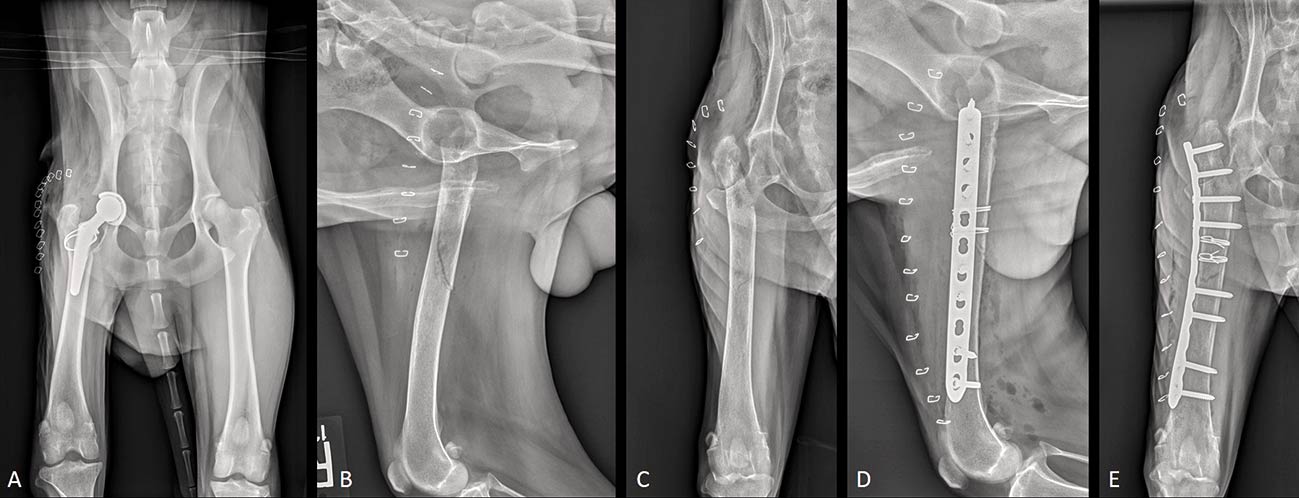
While NSAIDs remain an integral part of OA management, their potentially severe side effects are being increasingly recognised, as is the fact many dogs do not achieve a pain-free state with their use in isolation. Many additional analgesics can be added to assist with this, but even in the face of multimodal therapy, a proportion of dogs continue to experience chronic pain. Total joint replacement is available for some joints affected with OA and can be expected to relieve the associated discomfort, but these are aggressive surgeries with associated potential for complications (Figure 2) and expense some owners cannot conscience.
Extensive research continues to be performed in the quest for additional pharmacologic options with either different mechanisms of action or more targeted actions in comparison to NSAIDs. Grapiprant, diacerein and anti-nerve growth factor antibody represent three of the promising medications that may become valid options in the battle against OA-related pain in the future.