23 Oct 2017
Francesca Doria discusses the causes, signs, diagnostic procedures and treatment options relating to oedematous vaginal mucosa protrusion in canine patients.

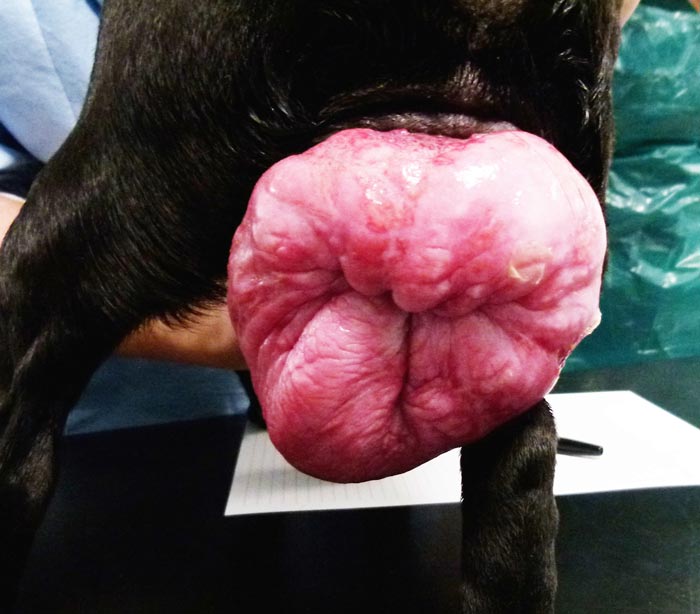
Vaginal fold prolapse is defined as the protrusion of oedematous vaginal mucosa into the vaginal lumen and, often, through the vulvar cleft. This disease represents an exaggerated response of the vaginal mucosa to the oestrogen stimulation that characterises the follicular phase of the oestrus cycle. It is an uncommon condition and affects young and intact bitches primarily during proestrus or early oestrus.
The incidence is higher in large breed dogs – especially brachycephalic breeds – and recurrences are very common if affected bitches are not properly treated. The most common clinical signs are the presence of a mass of varying sizes protruding from the vulvar cleft and vulvar discharge or bleeding.
By performing a careful vaginal examination and palpation, it is possible to classify a vaginal fold prolapse in three types, based on the degree of protrusion. Differential diagnoses include vaginal and vulvar tumours, clitoral hypertrophy, true vaginal prolapse, urethral neoplasia and uterine prolapse. Different treatment options are available and depend on the extent of the fold prolapse, the purpose for which the animal is kept, and the stage of the oestrous cycle the bitch is exhibiting at the time of diagnosis.
Vaginal fold prolapse (VFP) is defined as the protrusion of oedematous vaginal mucosa into the vaginal lumen, often through the vulvar cleft. The condition has been traditionally referred to as vaginal hyperplasia, oestral hypertrophy, vaginal prolapse, vaginal eversion and vaginal protrusion.
Differently from other species, it is not a true organ prolapse as only the mucosa is involved. Also, the prolapsed tissue is histologically characterised by oedema and fibroplasia, and is no more hyperplastic than the rest of the vaginal mucosa under oestrogen stimulation. Because of this, the terms vaginal oedema and vaginal fold prolapse should be used.

During the follicular phase of the oestrous cycle, the vaginal mucosa physiologically becomes oedematous, hyperaemic and keratinised due to oestrogen influence. In patients presenting a VFP, these changes are more severe as a result of an exaggerated response of the mucosa to the oestrogen stimulation. Oestrogens, therefore, play the major role in the pathogenesis of this condition and this can be confirmed by the fact:
The reason why, in some bitches, there is this increased reaction is undetermined.
Even if hyperoestrogenism hasn’t been identified in affected bitches, an excessive oestrogen production from cystic ovaries has been suggested as a potential cause.
Administration of exogenous oestrogens for therapeutic purposes has been reported to be a contributory factor in the development of this condition.
VFP can also affect bitches during the final weeks of pregnancy, when the concentration of serum progesterone declines and the concentration of serum oestrogen increases. In this phase, oestrogens cause relaxation of the pelvic ligaments, vulvar and perivulvar musculature and associated tissues. The aetiology in these patients is considered a combination of pregnancy-related elevated oestrogen and increased intra-abdominal pressure.
This condition is uncommon and usually affects young (younger than two years old) and intact bitches, primarily during proestrus or early oestrus. It has also been reported during late pregnancy, after administration of oestrogenic drugs and, on rare occasions, it can recur later in the same cycle at the end of dioestrus.
If the affected bitch is not properly treated, it is common to observe recurrences, characterised by different severity, during each oestrous cycle.
The incidence of VFP is higher in large breed dogs – especially brachycephalic breeds (for example, boxer, bullmastiff and bulldog). Some families of purebred dogs were reported to have an increased risk to develop the disease and a potential hereditary component was suggested. For this reason, it should be considered if affected bitches should be bred.
The most common clinical signs are the presence of a mass of varying sizes protruding from the vulvar cleft and vulvar discharge or bleeding. Despite the fact the oedematous tissue lies over the external urethral orifice, urine flow is rarely impeded and anuria, dysuria, pollakiuria or stranguria are uncommon clinical signs. Other less commonly reported clinical signs include increased perineal licking, perineal enlargement and swelling, tenesmus and inability or unwillingness to breed.
By performing a careful vaginal examination and palpation, it is possible to classify a VFP in three types, based on the degree of protrusion:
In cases of type II or type I VFP, the vaginal lumen is dorsal to the everted mucosa, while in cases of type III, it is centrally located. The urethral orifice is always localised ventrally to the fold prolapse (Figure 3) and the rest of the vaginal mucosa appears normal.
Vaginal cytology and measurement of serum progesterone (P4) concentration are useful to confirm the stage of the oestrous cycle:

No abnormalities are usually seen in serum chemistry values or hormonal profiles of affected bitches. Thoracic/abdominal radiographs and abdominal ultrasound are rarely necessary unless to investigate for metastasis due to the suspicion of a neoplasia or visceral herniation. Organs that can be herniated are the bladder, colon and uterus.
Fine-needle aspiration or punch biopsy is recommended in middle-aged and older bitches to differentiate from a neoplastic lesion.
A vaginal protruding mass is a clinical finding that characterises several genital diseases. Detailed patient signalment, reproductive history, clinical examination, site of mass origin, changes of mass with the oestrous cycle, hormonal assay and vaginal cytology are important to differentiate these conditions. Diagnoses for VFP include:
Tumours usually affect older bitches, do not have a specific localisation inside the vaginal lumen and do not regress, at least partially, during the luteal phase as VFPs do. A true vaginal or uterine prolapse mainly occurs during the parturition or shortly after.
Different treatment options exist and depend on the extent of the fold prolapse, the purpose for which the animal is kept and the stage of the oestrous cycle the bitch exhibits.
The conservative approach is usually chosen for breeding bitches and when owners refuse any type of surgical procedure to the reproductive tract. The aims of this treatment are:
This can be accomplished using lubricating jelly, topical antibiotic or antibiotic-steroid ointments, artificial tears, warm saline solutions, protective pants and an Elizabethan collar. Attention must be paid to the edges of the collar to avoid further trauma to the mass, and potentially irritating bedding should be removed. Furthermore, the perineal and vulvar skin needs to be kept dry as it may be subject to maceration.

Vaginal smears and serum P4 measurements should be continued periodically during the conservative approach to monitor the cycle of the bitch.
The use of gonadotropin-releasing hormone or human chorionic gonadotropin to shorten oestrus and induce premature ovulation has been used with limited success.
Progestagens have been suggested for treatment and prevention, but can have side effects, such as cystic endometrial hyperplasia or endometritis, leading to pyometra – especially when administered during an oestrogen-dominated phase.
The conservative approach is not ideal, as this condition tends to recur – even if with different degrees of severity – every oestrus cycle.
AI may be considered when a valuable bitch will not allow intromission and the owners insist on breeding. The condition will resolve spontaneously as soon as the pregnancy starts, and it is unlikely to recur and cause dystocia at the time of parturition.
If a fold prolapse develops just prior to whelping, the conservative approach is, in general, used and parturition can normally take place without problems.
Ovariectomy or ovariohysterectomy is the treatment of choice for non-breeding bitches presented with uncomplicated type II or type I VFP as it ensures a permanent regression of the condition and eliminates the risk of recurrence.
Spaying should be performed in anoestrus as during oestrus the risk of haemorrhage is higher and during the luteal phase of the cycle pseudopregnancy symptoms – even if just transient – can be induced.
During surgery, it is good practice to take a biopsy of the mass to rule out neoplasia.
While waiting for the best moment to perform the ovariohysterectomy, the patient can be managed using a conservative approach as aforementioned. Prognosis after ovariohysterectomy is excellent for non-traumatised and non-ulcerated cases, and regression of the oedematous tissue usually occur within several days to three weeks.
Resection can be performed either with or without ovariohysterectomy and should be considered when:
The prolapsed mass is usually highly vascularised and surgery is generally characterised by considerable blood loss.
Prior to surgery, a purse-string suture is placed around the anus to keep the surgery field clean of contamination.
Urethral catheterisation is performed to identify the urethra during the procedure and thus prevent damage (Figure 4). The patient is placed in sternal recumbency with the pelvic limbs and perineum suspended over the end of the surgical table. Padding should be used to prevent nerve or muscle damage.
An episiotomy procedure can be considered to better visualise the vagina and urethral orifice, and exteriorise the mass.
The surgical approach is different whether the VFP is a type II or III. With type II, the mass is resected at the level of the base as close as possible to the vaginal floor.
A fusiform incision is made around its base and the resulting mucosal defect is closed with monofilament absorbable suture in a continuous or interrupted appositional pattern.
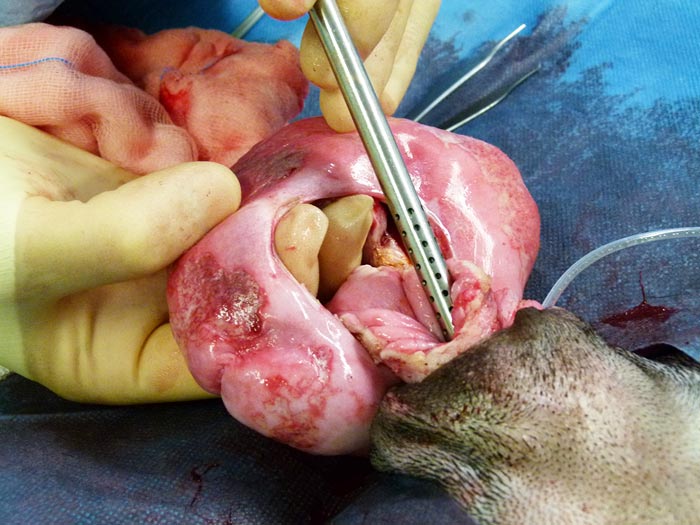
In cases of type III, the vaginal lumen lies within the centre of the prolapsed tissue. To help with the identification of the lumen, a Poole Suction Tube tip can be introduced through the centre of the mass.
A staged circumferential incision is made; a 25 per cent full-thickness incision of the mass is performed and the adjacent mucosal edges are apposed with simple interrupted absorbable sutures, followed by another 25 per cent until the full circumference of prolapsed tissue is resected (Figures 5 and 6).

During both procedures, severe bleeding during surgery can be controlled with electrocoagulation, resecting and suturing in phases, and by placing horizontal mattress suture before making the incision.
Following surgery, urination should be checked daily to make sure the urethra or the urethral orifice have not been damaged.
Correct haemostasis during surgery should prevent post-surgical bleeding. However, if the surgical area continues to bleed after surgery, a vaginal tampon may be placed for up to 12 hours. An Elizabethan collar is placed immediately after surgery to prevent self-trauma. Opioids and NSAIDs are used to provide analgesia and reduce postoperative swelling.
A bitch presented with VFP should be cured, as prognosis is excellent – even with the presence of prolapsed necrotic tissue. Prognosis is more guarded if a true prolapse is present, which could involve abdominal organs.