3 Mar 2026
Phil Witte BSc, BVSc, CertAVP(GSAS), DSAS(Orth), MRCVS claims that the surgical management of this issue is at a crossroads and reviews the options available.
Philip Witte
Job Title
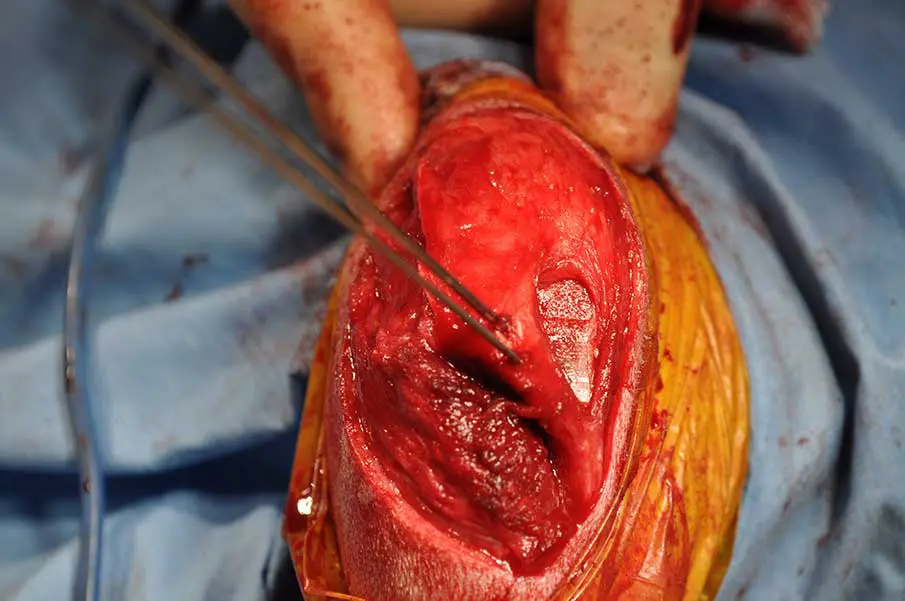
Figure 1. Rectangular block recession trochleoplasty demonstrated in intraoperative photographs of the distal femur of a dog with patellar luxation viewed through a lateral parapatellar arthrotomy. Left: note almost complete absence of concavity in trochlea. Centre: slightly converging parallel osteotomies made at periphery of hyaline cartilage. Right: rectangular block has been removed, further bone has been removed from the ostectomy site and then the block has been replaced, now recessed, leaving enhanced trochlear ridges.
Patellar luxation (PL) remains one of the most commonly diagnosed orthopaedic conditions and one of the most commonly performed elective orthopaedic surgeries in dogs. PL is typically to the medial side, and this article will focus on medial patellar luxation.
Despite familiarity with this condition, the aetiology remains uncertain and surgical management continues to generate debate – particularly regarding the increasingly understood skeletal deformities.
PL should be regarded not as a primary disease entity, but as a clinical manifestation of abnormal hindlimb development. Anatomical abnormalities, which have been implicated in the abaxial orientation of the quadriceps mechanism, include a shallow trochlear groove, medial tibial tuberosity location, distal femoral varus and internal rotation of the tibia with respect to the femur.
Traditional surgical approaches have emphasised a “menu” of techniques – trochlear groove deepening, tibial tuberosity transposition (TTT) and soft tissue imbrication or release – often applied in combination. While many patellas can be stabilised with these interventions, complication rates remain significant, with recurrence of luxation and other postoperative complications reportedly affecting 10% to 30%.
In a previous article for this journal (VT54.51), the rationale for addressing femoral deformity was explored. This article builds on that discussion by reviewing surgical options, with emphasis on recognising the anatomical abnormalities of the individual dog and selecting procedures accordingly.
In 2006, Arthurs and Langley-Hobbs published a paper reviewing outcomes of 109 PL surgical procedures (13% major complications, requiring further surgery). This 20-year-old study can still provide a sound framework for evaluating current practice.
A more recent retrospective study demonstrated a rate of 18.5% major complications, despite an increased awareness of femoral deformity by that time (Cashmore et al, 2014) – a disappointing worsening of outcomes from one decade to the next.
Complications for PL surgery include those we could describe as mechanical failures: re-luxation and implant failure (due to implant overload); and biological failures: delayed union, infection and persistent lameness (the latter potentially being associated with ongoing malalignment between the trochlear groove and the functional direction of the quadriceps mechanism). Arthurs and Langley-Hobbs suggested that a standardised surgical recipe may not reliably address the pathological diversity of PL. Failure to recognise and/or adequately correct underlying skeletal deformities will result in poorer outcomes. This observation aligns with increasing recognition that patellar luxation is a clinical manifestation of abnormal limb development.
Determining which factors contribute significantly in the individual dog is fundamental to selecting the appropriate surgical intervention.
Soft tissue techniques include release of tight parapatellar tissues on the medial aspect and imbrication of loose parapatellar tissues on the lateral aspect (either by overlapping or removing an ellipse of tissue during closure). However, soft tissue procedures do not address quadriceps malalignment. When used as the sole intervention, they are associated with high rates of recurrence.
Interestingly, Arthurs and Langley-Hobbs reported an increase in complication rate in cases with medial soft tissue release. The author suggests this data is interpreted as an increase in PL grade being more likely to require release and more likely to result in complications, rather than that release is in itself a cause of complications.
Soft tissue techniques should be viewed as adjunctive, refining patellar tracking alongside quadriceps realignment, rather than compensating for uncorrected skeletal deformity. It is the author’s experience that with the higher grades of PL, medial release (Figure 1) can be critical to permit reduction of the patella during surgery, while reliance on lateral imbrication to maintain quadriceps alignment is unlikely to provide durable patellar stability.
Trochleoplasty has historically been considered a cornerstone of PL surgery. Techniques include wedge recession, rectangular block recession (Figure 1), abrasion trochleoplasty and chondroplasty in immature dogs. The rationale is straightforward: a deeper groove provides greater resistance to luxation of the patella.
Trochlear hypoplasia occurs secondary to PL during growth and does not represent the initiating pathology. If quadriceps alignment is restored, the patella may track adequately within a relatively shallow groove. Furthermore, trochleoplasty is not benign. It causes (peripheral) hyaline cartilage damage, exacerbating osteoarthritis; therefore, some authors have questioned the necessity, and even the desirability, of routine groove deepening.
Linney et al (2011) reported acceptable outcomes in dogs treated with tibial tuberosity transposition (and lateral imbrication), but without trochlear groove deepening. However, when the numbers are reviewed, re-luxation was present in 19.8% of cases in the Linney study, despite the case selection being somewhat skewed toward lower-grade PL. The comparable re-luxation rate of 8% in Arthurs and Langley-Hobbs (2006; where groove deepening was performed in the majority of cases) would suggest groove deepening is important in a significant proportion of cases. This point was considered sufficiently important that in both Arthurs and Langley-Hobbs (2006) and Cashmore et al (2014), the abstracts include words to this effect.
Groove deepening seems to be an integral component of the surgery for PL in many cases, but if it is to be considered selectively, rather than as a default procedure, we have yet to establish guidelines for evaluation of what constitutes appropriate groove anatomy.
TTT aims to realign the quadriceps mechanism by repositioning the patellar tendon insertion (Figure 2). TTT can be highly effective. It is also worth noting, however, that most dogs with lower-grade PL do not have a medially positioned tibial tuberosity (Yasukawa et al, 2016), so TTT is not truly addressing a deformity (medial tibial tuberosity), but is actually causing one (lateral tibial tuberosity). This is not inherently problematic, provided it is performed within its biomechanical limits. TTT can compensate for deformities including femoral varus, femoral torsion and stifle joint rotation to a point.
Failure to address these deformities specifically may risk creating excessive stresses at the tibial tuberosity osteotomy site, contributing to complications such as avulsion or delayed union (Arthurs and Langley-Hobbs, 2006). Additionally, it could be argued that compensation for femoral or stifle deformities with TTT could mean continued non-parallelism between the trochlear groove and the direction of tracking of the patella.
TTT should be regarded as a component of alignment correction, not a substitute for addressing femoral geometry when significant deformity exists. It is reasonably considered the mainstay procedure for PL surgery.
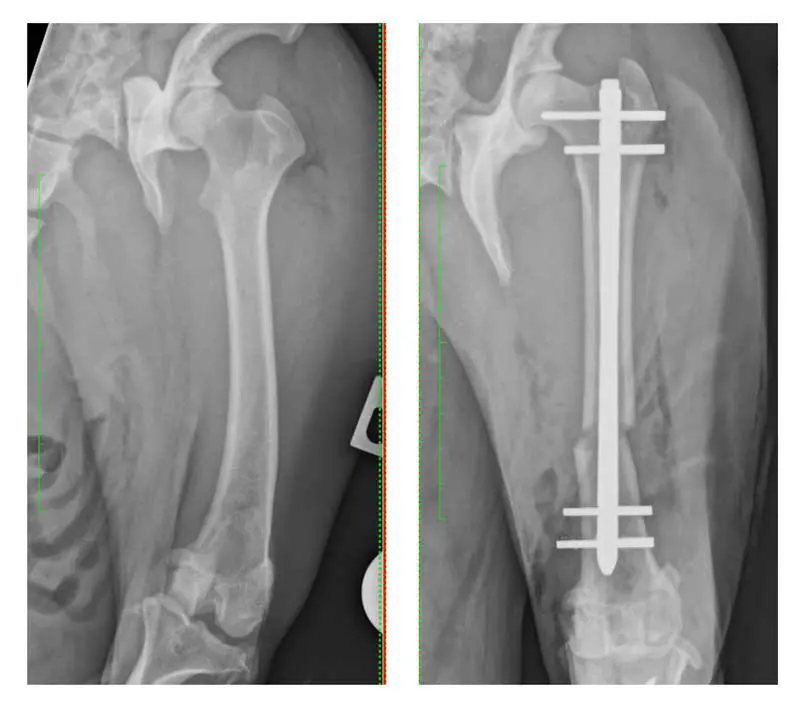
Femoral deformity plays a central role in many cases of PL. Swiderski and Palmer (16 stifles in 2007) and Brower et al (66 stifles in 2017) described the retrospective outcomes for dogs undergoing correction of distal femoral varus deformity (Figure 3) as a component of management of medial PL.
Lee et al (2020) further characterised the correlation between PL and distal femoral varus using a cadaveric study, identifying an anatomical lateral distal femoral angle of more than 103° as the severity of varus beyond which deformity correction should be considered.
Given the nature of the data, this should be considered a pragmatic threshold, rather than an absolute indication. An added complexity is present, as femoral deformity is often multiplanar, involving combinations of varus and torsion, and 3D imaging is more sensitive for identifying abnormal anatomy. Brower et al (2017) highlighted the role of CT-based planning in identifying torsional deformities not evident on radiographs.
Distal femoral osteotomy allows direct correction of femoral alignment and is increasingly accepted in dogs in which deformities exist (Figure 3). Techniques include closing wedge, opening wedge and dome osteotomies, often stabilised with plate/screw combinations. Corrective osteotomy is not without risk. It increases surgical time, cost and technical demand, and complications such as delayed union or implant failure can occur. However, when performed appropriately, it addresses the root cause of patellar maltracking.
In the earlier literature regarding high-grade PL, a rotational deformity in the stifle joint, with the tibia internally rotated with respect to the femur, is often described (Figure 4).

Compensatory external torsion is often present in the tibia. Derotation of the stifle is under-reported in the literature (Chen et al, 2021; Petazzoni et al, 2026). The author’s caseload includes a large number of cases with this particular deformity, which is frequently addressed through stifle derotation as a standalone intervention or in combination with trochlear groove deepening. Further data regarding stifle rotational deformity and what may be achieved through derotation is required, and will hopefully become more available in the near future.
Theoretically, failure to recognise femoral torsional and stifle rotational deformities risks performing technically successful surgery that does not restore normal biomechanics.
In other words, an extreme TTT may compensate for distal femoral varus and/or stifle internal rotation by encouraging the patella into the trochlear groove, but the direction of travel of the patella may not match the long axis of the trochlear groove. This may be assumed to be uncomfortable, but no evidence exists to show that extreme TTT to compensate for femoral or stifle deformities results in poorer outcomes.
In fact, no correlation was found between measures of femoral varus angle and any complications (including re-luxation) in a retrospective study of 87 canine stifles undergoing standard PL surgery with no femoral deformity correction (Perry et al, 2017). The authors of that study concluded that femoral varus deformity correction may be unnecessary to restore patellar stability in dogs.
Whether a superior outcome in terms of clinical function can be achieved by addressing femoral deformities (where they exist) rather than extreme TTT remains undocumented, but is assumed in the studies in which deformity correction is recommended (Figure 5). In this case, the adage that absence of evidence is not evidence of absence may be applicable. Published objective outcomes data is lacking for now.

One of the most significant recent developments in understanding PL is the application of CT imaging. Three-dimensional imaging (CT) and computer modelling allows us to assess bone anatomy and stifle joint alignment with greater accuracy than 2D imaging.
However, as we learn more about the anatomy and how to assess it, we start to need protocols for measurement of the aspects we feel are important, as well as reference ranges for these measurements to determine what is normal and what is not.
As the depth of understanding improves and data is published, we can hope that the “art” aspect of PL surgery will reduce and options will be based more on geometric rigour.
Agreed protocols for what to measure and how among the profession do not exist, and complexity increases when, for example, awake CT (Tomo et al, 2022) is added into the fray, apparently giving greater insight than static CT can.
CT imaging enables accurate measurement of:
While CT is not necessary for every case, it is increasingly difficult to justify complex reconstructive surgery without detailed understanding of limb geometry. As access to advanced imaging improves, expectations of surgical planning will continue to evolve.
Obviously, cost, access and the learning curve of the individual charged with case management remain reasonable real-world limitations to the universal uptake of CT for PL case management.
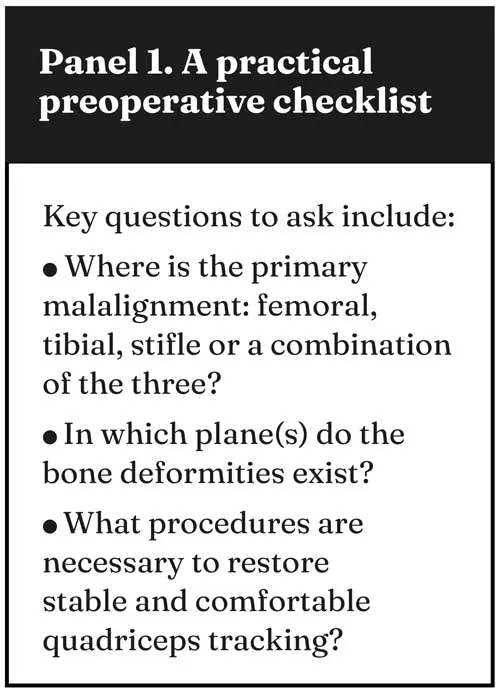
Perhaps the most important message emerging from the literature is that no single surgical approach is universally appropriate. The temptation to apply a familiar combination of procedures should be resisted in favour of a structured assessment of each dog’s anatomy.
Answering the questions in Panel 1 may allow the surgeon to tailor the surgical plan, potentially reducing unnecessary procedures and hopefully improving outcomes.
The surgical management of PL in dogs is at a crossroads. Traditional techniques remain valuable, but their limitations are increasingly apparent. The literature reviewed here supports a shift away from routine, standardised procedures toward individualised, anatomy-driven surgical planning. In this way, we may hope to reduce the stubbornly high rate of complications.
CT does not have to be performed for every single case, but it has the power to more definitively identify deformities to aid surgical planning.
Recognising femoral, tibial and stifle deformity, selecting appropriate corrective interventions, and questioning the routine use of trochlear groove deepening represent important steps in improving outcomes.
Ultimately, the goal is not simply to keep the patella in the groove, but to restore a limb that functions as close to normal as possible.
Phil Witte has many years of experience working in orthopaedics-only referral-level veterinary practice. He holds an RCVS certificate in small animal surgery and an RCVS diploma in small animal orthopaedics. Phil is a director at Wessex Veterinary Orthopaedics and performs peripatetic orthopaedic surgery via Rata Veterinary Surgery around the south coast of England. He is co-author of Feline Orthopaedics (second edition) and has interests in trauma and angular limb deformity management.