2 Sept 2025
This article was reproduced based on a guideline written collaboratively with Dômes Pharma by: Rachael Grundon, Bsc, VetMB, CertVR, CertVOphthal, MANZCVS (Surgery), FANZCVS (Ophthal), DipECVO, MRCVS; Maria-Christine Fischer, DipECVO, FHEA, MRCVS; Jens Fritsche, DipECVO; Alexandre Guyonnet, DipECVO; Fernando Laguna Sanz, DipECVO; and Sophie Amiriantz, MSc, DVM
Vet Times
Job Title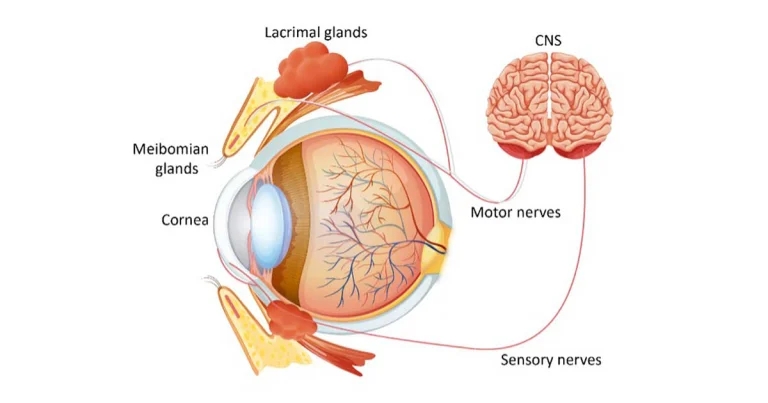
Figure 1. The Tear film unit (note: the goblet cells are not labelled and are found within the conjunctiva). Image: © Dômes Pharma
Dry eye disease (DED, keratoconjunctivitis sicca/KCS) is a disease syndrome of the ocular surface arising from dysfunction of one or more components of the tear film unit (see Figure 1), that is the secretory glands, ocular surface, eyelids and the motor and sensory nerve supply, which create and distribute the preocular tear film. This results in ocular surface inflammation, discomfort and damage, which can be mild to severe.
We tend to place DED into one of three main types:
Tears are present over the surface of the eye as a triple-layered film (see Figure 2).
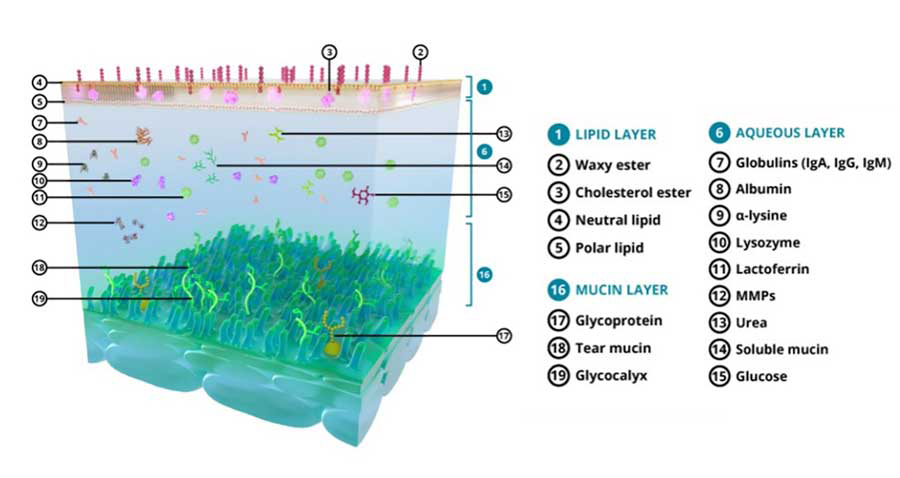
The outer oily or lipid layer is provided by the meibomian glands, located at the edge of the eyelids. It delays tear evaporation and evens out the surface of the tear film.
The middle layer is the aqueous layer, which is secreted by the lacrimal glands including the gland of the third eyelid. It is the thickest layer of the tear film, and provides nutrients, oxygen and microbial protection to the ocular surface. It is also responsible for hydration of, and the smooth movement of, the eyelids over the cornea.
The third, innermost layer is the mucin layer, which is produced largely by the conjunctival goblet cells. The mucins it contains are responsible for the adhesion of the tear film to the ocular surfaces.
Tears are continuously spread over the surface of the eye in a uniform, thin layer by the constant action of the eyelids (and nictitans) during blinking and removed via the nasolacrimal system.
The precorneal tear film serves several functions, including:
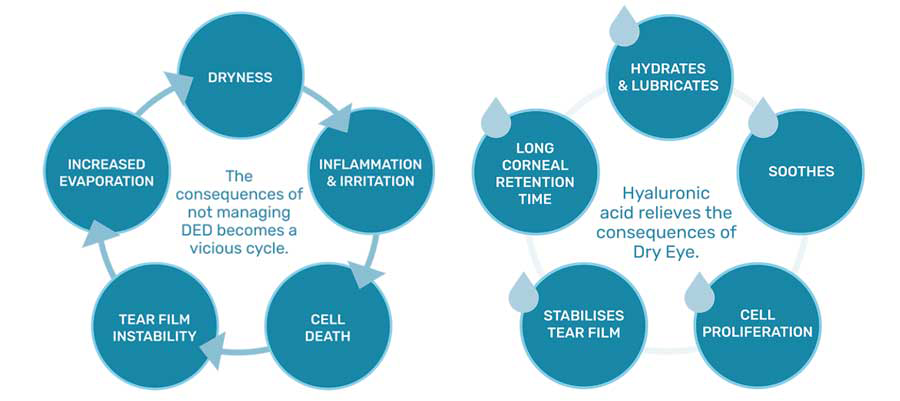
Abnormalities in either the quantity or quality of any tear component (lipid, aqueous, mucus) compromises these tear functions.
Hypertonicity and dehydration of conjunctival and corneal epithelia are initial pathophysiologic events, lack of appropriate lubrication results in frictional irritation of the ocular surface, toxic tissue metabolites may accumulate on the ocular surface and microorganisms more readily colonise affected eyes – all resulting in an increased incidence of ocular surface infections and pathology.
Various aetiologies have been described in dogs and the DAMNIT list can be used systematically to investigate the causes of reduced tear production:
One should note that the DAMNIT list does not rank causes in order of severity or frequency.
The dysfunctional factors can be compounded by environmental conditions (such as pollens, wind) and trigger clinical signs in animals that were compensating until then.
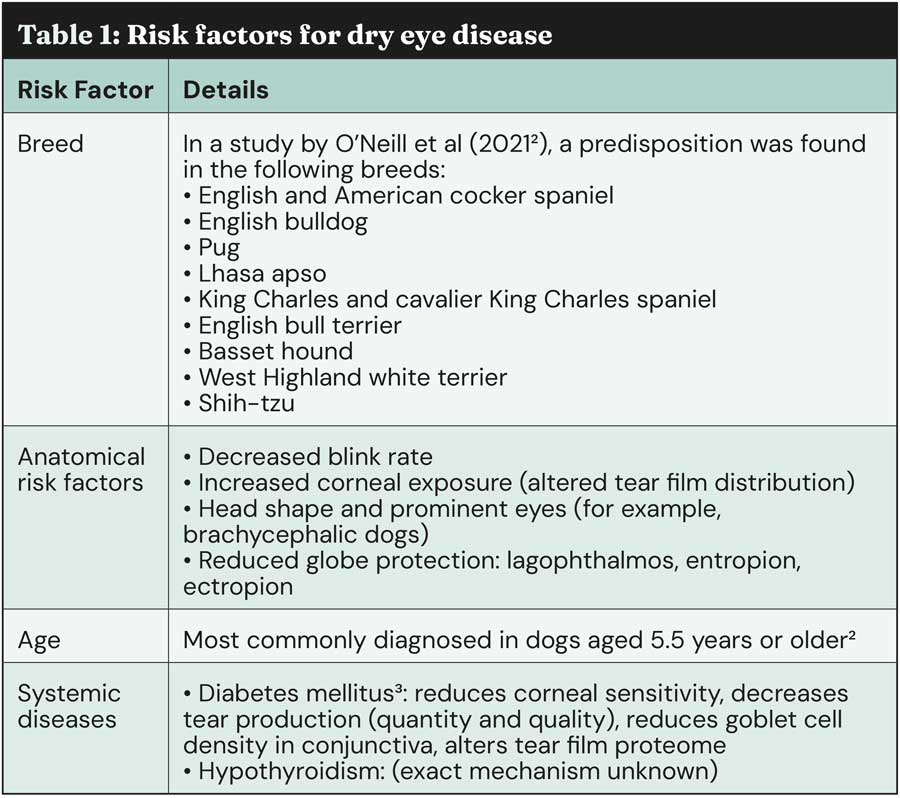
It is suggested that 1 in 22 dogs suffer with dry eye1, however, the true prevalence of DED is hard to ascertain because of under-diagnosing. However, some risk factors (See Table 1) have been clearly identified and should be seen by GP vets as red flags prompting them to further investigate the possibility of DED.
The presence of even just one of these signs should trigger dry eye investigation:

The diagnosis is based on the history, the presence of compatible clinical signs and supported by diagnostic tests.
A full physical examination and further investigation should be taken into consideration to rule out systemic underlying causes such as metabolic diseases.
A complete ophthalmic examination is necessary to assess vision, clinical signs of dry eye disease and neurological abnormalities. In addition, assessment of the nares for dryness is essential in diagnosing neurogenic dry eye.

The Schirmer tear test (STT) remains the standard means for quantifying aqueous tear production and diagnosing quantitative tear film deficiency. The STT should be performed on every patient with an eye complaint (unless a deep ulcer is present, in which case avoid or take great care). It should be performed first in the ophthalmic exam to avoid falsely high values from reflex tearing associated with examination of the eye, and prior to application of any topical agents.
Without touching the bent end, the STT strip is inserted into the lateral half of the lower conjunctival fornix. The strip remains in place for one minute and the readings are taken immediately after removal.
Values between 10-15 mm/min can be consistent with aqueous tear deficiency if compatible with clinical signs, values between 5-10 mm/min are highly suspicious and values of less than 5mm/min are characteristic of severe disease. In case of doubt a re-examination should be scheduled for repeat measurement4.
Stains such as fluorescein can be used to assess the integrity of the epithelium and stability of the precorneal tear film. Tear Film Break Up Time (TFBUT) (see Figure 5) can be used to evaluate the quality and stability of the tear film and may be abnormal in the presence of a normal STT result. Lissamine green and Rose Bengal stains can further aid the diagnosis but are more commonly used in referral practice.

Assessment of the blink rate and effectiveness is especially helpful in brachycephalic dogs. In case of incomplete and infrequent blinking one must assume greater evaporative loss. Taking slow-motion videos can help identify incomplete eyelid closure.
When confronted with dry eye patients, the practitioner should remember to treat the patient as a whole, and not just the STT value.
Ocular pain, comfort and complications are as critical as tear production, if not more. Additionally, the owner will be more mindful of clinical signs than of diagnostic test results.
Recommendations for initial management include:
Involvement of the owner is essential in the management of DED: teaching them good practices of eye cleaning and treatment administration is essential. Making sure they understand improvement can take several weeks, and treatment is often life-long.
In the absence of response to first line treatment, owner compliance should be evaluated and referring your patient to, or obtaining advice from, a veterinary ophthalmologist is advised.
Dry eye disease, or keratoconjunctivitis sicca, results from the dysfunction of one or multiple structures of the tear unit, leading to clinical signs (mucopurulent discharge, recurrent conjunctivitis) along with compounding environmental conditions.
DED has many aetiologies, most frequently immune-mediated in dogs. Some risk factors such as breed, age or systemic diseases are red flags the GP should take into consideration.
The diagnostic process involves several steps, including quantification of tear production with a Schirmer tear test alongside assessment of clinical signs. Ciclosporin should be considered first-line treatment alongside tear supplements as an adjunct.
Owner compliance is critical in the success of DED management, and they must be fully aware that this is a chronic disease and that treatment must be continued for life.
To view Dômes Pharma’s Practical Ophthalmology, step-by-step guide, visit the website.
This article was reproduced based on a guideline written collaboratively with Dômes Pharma by: Rachael Grundon, Bsc, VetMB, CertVR, CertVOphthal, MANZCVS (Surgery), FANZCVS (Ophthal), DipECVO, MRCVS; Maria-Christine Fischer, DipECVO, FHEA, MRCVS; Jens Fritsche, DipECVO; Alexandre Guyonnet, DipECVO; Fernando Laguna Sanz, DipECVO; and Sophie Amiriantz, MSc, DVM