10 Feb 2026
Implementing geriatric screening is a strategic long-term investment that enhances clinical outcomes for ageing patients while securing practice revenue. By identifying silent pathologies early, clinicians can transition “healthy” seniors into managed care pathways, fostering client loyalty and driving consistent income through essential follow-up diagnostics...
Mike Davies
Job Title
Image: Chalabala / iStock
According to the British Geriatric Society, screening of elderly people involves a comprehensive geriatric assessment (CGA), which is a structured multidisciplinary approach offering gold standard care for older adults.
It is evidence-based, and increasingly recognised for its role in improving quality of care of older people across various pathways and health care settings (British Geriatric Society, online).
Screening of geriatric veterinary patients has been done in practice since the 1980s, with the first textbooks on the subject being published in 1995 and 1996 (Davies 1996; Goldstone and Hoskins 1995). The first scientific paper on geriatric screening in pets was published in 2012 (Davies, 2012).
The aims of geriatric screening of cats and dogs are:
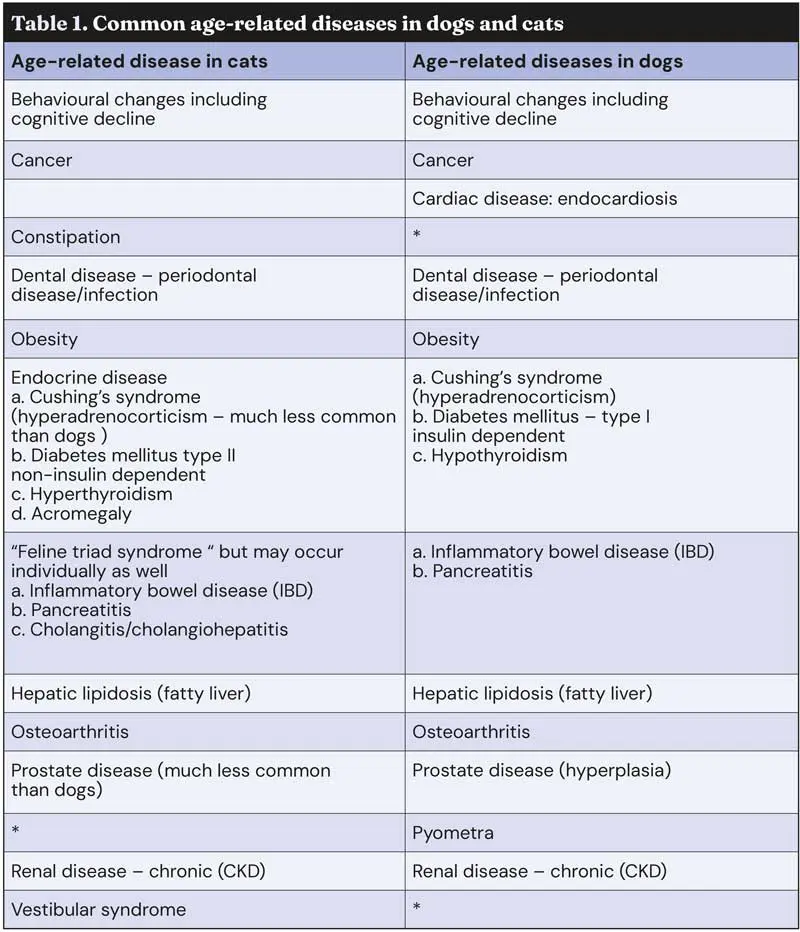
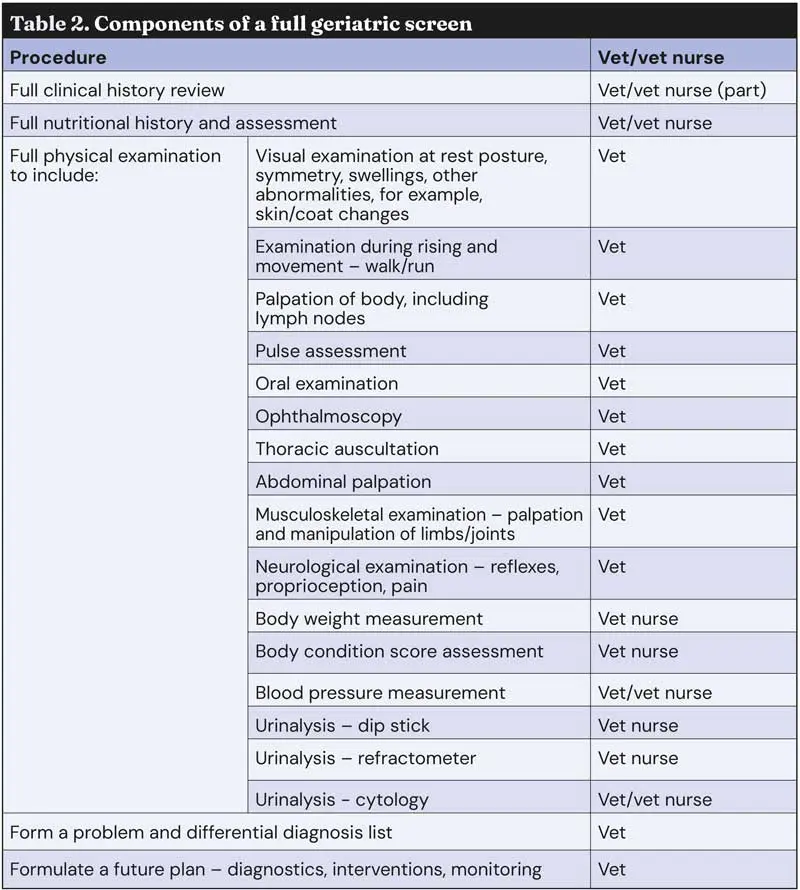
There is no point in doing a screen unless it rules in or out the presence of the main common age-related diseases (Table 1; Davies, 1996; Goldstone and Hoskins, 1995; Davies, 2012; Sturgess, 2024). Therefore, a geriatric screen must include a series of procedures (Table 2), some of which can be done by a trained veterinary nurse, but others can only be done by an experienced veterinary surgeon.
Please note, a geriatric screen is not a blood test; indeed, blood tests are invasive and should only be done when clinically indicated from the history or physical examination.
Ongoing research aims to produce a tool to help veterinary clinicians to maximise the value of geriatric screening (McKenzie et al, 2022).
The financial viability of a practice-run geriatric screening programme is determined by the costs of running the programme, which are mainly staff costs, and the income that can be generated from the pet owners who agree to participate.
In my experience, a full geriatric screen cannot be completed in less than 45 minutes, with an average of one hour.
In the most elderly patients with multiple co-morbidities it can take considerably longer. As can be seen from the procedures that need to be done (Table 2), most staff time, and therefore cost, will be for veterinary surgeon time.
It is valid to include urinalysis in the screen as abnormal findings can be expected from 66% of tests performed (Davies, 2012).
Any additional costs for diagnostic tests, for example imaging, will be charged direct to the client.
Over the years I have seen several ways in which fees have been charged for providing geriatric screening:
The full screen is done at no cost to the owner, but practice revenue is expected to offset this from additional diagnostic investigations (for example, blood tests, imaging) or medical/surgical interventions.
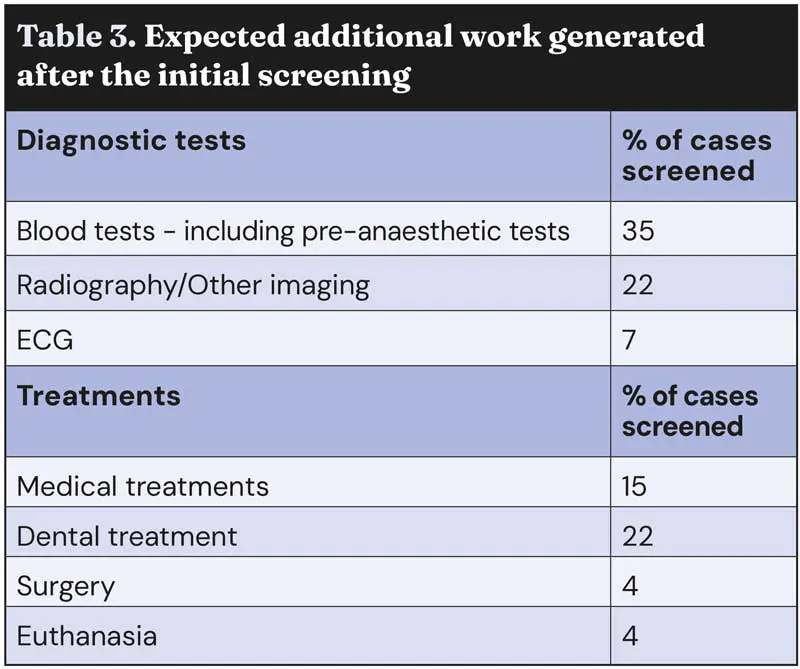
This is a valid strategy as additional diagnostic tests and/or interventions are likely in the majority of cases (Table 3). Indeed, in only 10% of cases are no new clinical findings likely to be identified from the screening process (Davies, 2012).
This approach also removes the initial barrier of asking an owner to pay a consultation fee when they may not think there is anything wrong with their pet other than normal ageing. Also, any further investigations or interventions deemed necessary after the screening should be covered by pet insurance policies.
If a client has patronised a practice for many years, staff should be prepared to provide an hour or so of their time once or twice during the lifetime of their pet, to reinforce the practice-client relationship.
Good client communication is necessary, however, because owners may not be happy – and practice motives may be questioned – if the initial consultation is offered free, but subsequently costly diagnostic investigations or medical/surgical treatments for hundreds of pounds are recommended.
This is a valid way of charging for the service, but would present a problem and be a barrier for some cost-conscious clients, and also clients who do not consider there is anything wrong with their pet.
The Society of Practising Veterinary Surgeons (SPVS) publishes a survey of its members’ fees at www.spvs.org.uk, but you need to calculate the actual costs for your practice based on your fee structure, bearing in mind most of the time allocated to do geriatric screening will be for vets, and only some of it for nurses.
I know one practice that successfully ran such a programme, but it had a wealthy client base, and the number of cases recruited was not that high.
This practice included some screens that were not necessarily clinically indicated – blood tests and survey radiographs. Under these circumstances, such investigations would likely not be covered by pet insurance policies.
Screening identifies a lot of new, serious conditions including, as in a study involving just 45 dogs (Davies, 2012):
These problems require further diagnostics, medical or surgical intervention (Table 3) with their associated revenue generation for the practice.
Geriatric patients require ongoing monitoring, repeat examinations, repeat prescriptions and sometimes further interventions.
Elderly pets should be examined at least once a year, if they have a chronic disease at least every six months, and if they have a serious disease every three to four months.
Owners may not comply with more frequent routine examinations. For most elderly pets, the practice can expect to have repeat business for the lifetime of the pet, but for this to happen continuity of care is required.
A successful client-practice relationship is less likely if there is inconsistency in the advice given to clients each time they attend the practice. In other words, the client should be able to see the same professional staff on each visit. Geriatric screening programmes are unlikely to work well if the pet owner sees a different nurse, or locum vet, each time they attend an appointment.

Geriatric screening is primarily for the health benefit of senior patients. It can and should be financially viable and worthwhile for practices that have spare capacity within their nurse and veterinary surgeon staffing levels, and with available space in which to carry out the consultations.
Other practices would need to calculate out a detailed cash flow forecast to justify running such a programme.
Geriatric screening should be regarded as a long-term investment in the patient primarily for its clinical benefits, but also to reinforce the practice-client bond.
For most patients, ongoing revenues can be expected from long-term medication and/or food sales, regular monitoring and repeat screening tests as recommended by independent organisations such as the IRIS Guidelines for CKD.
Mike Davies has worked in academia and private practice, and for several pet food manufacturers and pharmaceutical companies. He speaks internationally on clinical nutrition and geriatrics, and founded the original City and Guilds certificate in small animal nutrition, and the BVNA certificates in small animal and exotic nutrition.