24 Feb 2026
Imogen Johns BVSc, FHEA, DipACVIM, FRCVS discusses the options for recognising and managing these non-infectious syndromes in horses.
Imogen Johns
Job Title
Image: bagicat / Adobe Stock
The term equine asthma encompasses the syndromes of non-infectious inflammatory lower airway disease, with subcategories of mild/moderate and severe equine asthma being used to denote disease severity based on the presence or absence of clinical signs (at rest or at exercise) as well as cytological analysis of lower airway samples1,2.
Although the term is all encompassing, there is no evidence to suggest there is a continuum of disease, with horses suffering from mild-moderate disease progressing inevitably to becoming horses with severe equine asthma (sEA).
Inflammation within the lower respiratory tract results in an influx of neutrophils, bronchoconstriction and mucus accumulation. Treatments are aimed at minimising exposure to triggering allergens through environmental management as well as reducing inflammation and inducing bronchoconstriction using corticosteroids and bronchodilators as necessary.
Poor performance (in particular in horses exercising at speed) may be the only sign in horses with the mildest form of the disease. In these horses, there is evidence of airway inflammation on cytology of bronchoalveolar lavage fluid (BALF; typically an increase in the percentage of neutrophils, but in some cases mast cells and eosinophils)1. Horses affected by moderate equine asthma will also have an inflammatory response in BALF, but will additionally have clinical signs attributable to lower airway disease (cough, increased respiratory rate and effort, and abnormal lung auscultation), but these signs are only evident at exercise1.
Horses with sEA suffer from repeated cycles of disease and remission. During periods of disease exacerbation, horses with sEA will show varying degrees of laboured breathing (nostril flare, increased thoracic excursion and anal “pumping”), increased respiratory rate and abnormal thoracic auscultation (classically end expiratory wheezes). Some horses will lose significant amounts of weight if the disorder is poorly controlled, presumably due to the increased work of breathing and/or less time spent eating due to the laboured breathing.
During clinical remission, if the disease is well controlled, clinical signs should be absent, although some horses will continue to show signs at exercise (cough and poor exercise tolerance) and abnormal auscultation may persist especially if a re-breathing bag is used. Horses are typically afebrile, and if a nasal discharge is present, it is mucoid rather than purulent.
Confirmation of the diagnosis should be pursued by endoscopy and cytological evaluation of BALF. If the horse is showing marked respiratory signs, delaying these tests may be sensible as some horses do not tolerate the procedure well when significant bronchoconstriction is present.
BALF, rather than a tracheal wash aspirate, is preferred, as the disorder is associated with small/distal airway pathology (which is the site sampled during a BAL) rather than a mixed small and large airway sample (tracheal wash). Historically, a poor correlation between tracheal wash and BALF cytology has been shown, and thus, when possible, a BAL should be performed3. The procedure can be performed endoscopically or via a BAL tube, with neither method shown to be superior.
A neutrophil count of greater than 20% of BALF cells is considered consistent with a diagnosis of sEA, although this number is somewhat debated between researchers, with values above 5% or 10% considered abnormal in some studies. Interestingly, in human asthma, up to a third of patients diagnosed with asthma did not actually have the disease (in most cases due to lack of appropriate diagnostic testing or interpretation of those tests) suggesting that the diagnostic challenges in equine asthma are not unique.
Despite marked airway inflammation, systemic (blood) markers of inflammation are typically not raised in horses with sEA. Should these markers be raised and/or the horse is febrile, an infectious respiratory disorder should be suspected and culture of a percutaneous tracheal aspirate may be warranted.
Equine multinodular pulmonary fibrosis (EMPF) is a rare disorder that can cause clinical signs similar to sEA. Horses can also be intermittently febrile and may have increased inflammatory markers. The disease is typically diagnosed following lack of response to treatment for suspected sEA and/or bacterial respiratory disease with radiographs showing a typical nodular pattern.
As triggers for sEA are known to exist in hay, straw and associated organic dust, it follows that the most effective long-term management strategy is antigen avoidance4. There is good evidence to show that in horses with sEA, horses can be effectively treated and remain in remission with normalisation of BALF neutrophilia, reversal of bronchoconstriction and reduction in airway remodelling when housed at pasture and fed a pelleted diet5,6. In horses with mild-moderate EA, the evidence is less clear, but similar recommendations exist1.
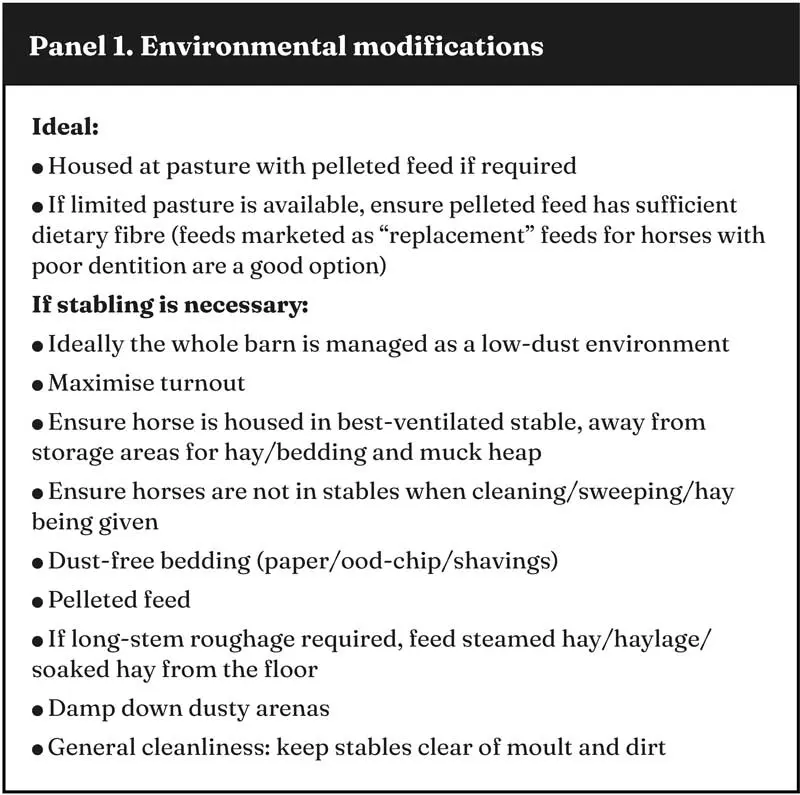
However, for many clients, this type of management is not possible or desirable, and thus, strategies to optimise the environment of affected horses while working within the constraints of the housing available for the horse must be implemented. While a holistic approach to dust reduction is important, what happens in the horse’s “breathing zone”, namely around the nostrils, appears to be the most important area to optimise.
As such, if only one change can be made, forage type should be the focus. However, bedding type, location of the horse’s stable within the barn, cleaning/mucking out schedules and location of storage of bedding and forage are all areas that should be evaluated to limit exposure of asthma-affected horses to airborne allergens in dust5,6.
It is important to thoroughly inspect the horse’s environment, as owners are not always aware of how these factors might impact the amount of dust inhaled (Panel 1). Owner compliance with recommended management strategies has been explored in two studies, one that recommended general “dust reduction” strategies7 and one that was more specific, listing six points that owners should address8.
Not surprisingly, (self-reported) owner compliance was greater in the first study, and was considered “poor” (less than two out of six points addressed) in the latter. Although the results of these two studies may appear somewhat contradictory, in essence they both highlight the desire of owners of sEA-affected horses to reduce allergen load and the challenges of putting this into practice.
Yard visits organised with the aim of determining how best to modify an individual horse’s environment while working within the limitations of the facility can be very beneficial and sometimes highlight previously unseen solutions. For example, an owner may be bedding their horse on dust-free shavings, feeding steamed hay and allowing for turnout during times when the yard is being swept, but the horse’s stable is located next to, and shares an air space with, a dusty arena. Simply moving the horse’s stable location may make a significant difference to the air quality, and, thus, the clinical signs in this horse.
The triggers for sEA are known to exist in hay and associated organic dust8. Regardless of the type of forage fed, every effort should be made to ensure that it is also of good quality, with no visible mould. Dry, mouldy hay is used in experimental studies to induce disease in asthmatic horses, with even good-quality hay having high levels of respirable dust. Respirable dust and mould levels can be decreased by steaming or soaking hay, or by feeding haylage. However, it is just as important that these processes are properly performed.
Soaking of hay can significantly reduce respirable dust, but prolonged soaking (longer than 60 minutes) can result in leaching of nutrients, and at even ambient temperatures (16ºC) can also result in increased microbial contamination of the hay. Reducing the water-soluble carbohydrate content of the hay is advantageous when feeding to overweight horses or those at risk of laminitis, and in one study soaking for nine hours, then steaming the hay, was the most effective method for both reducing water-soluble carbohydrates and microbial contamination in hay10.
For asthmatic horses that do not require weight control, hay should only be soaked for 10 to 60 minutes and fed straight away, which should allow for maximal reduction of dust while conserving the nutrient quality of the hay and minimising microbial growth.
Haylage is a conserved forage that is harvested at a higher moisture content than hay and can reduce exposure of respirable dust by 60% to 70% compared to dry hay.
Steamed hay can reduce respirable dust release in vitro by 95% and bacterial and mould content by 99%9. Commercially available steamers have spiked manifolds that pushes the steam into the hay and allows for appropriate temperatures to be maintained (temperatures of more than 90ºC for longer than 10 minutes being required to kill mould, for example). “Home-made” steamers are unlikely to reach sufficient temperatures for penetration of the hay, and may in some cases even exacerbate mould growth.
Steamed hay is often preferred by owners (and some horses), as soaking can be challenging – especially in winter – and is unpalatable to some horses. Steamed hay feeding was shown to have beneficial effects on clinical scores, BALF neutrophilia and lung function in horses during sEA exacerbation, although the effect was more pronounced when a purely pelleted diet was fed11. While steaming of hay is beneficial in many horses, it may not be appropriate for all horses. A 2025 study showed a mild, but significant, deterioration of lung function and inflammation in horses with sEA when fed steamed hay compared to dry hay for four weeks12. The authors suggested the lack of differences with dry hay could be due to the unexpectedly mild exacerbation during this study. A second study also showed no consistent improvements in respiratory signs in horses fed steamed hay13. As such, if clinical signs persist or worsen when a horse is changed to steamed hay, haylage or soaked hay (or pasture and a pelleted feed) should be used.
Ideally, low dust or “dust-free” bedding should be used if horses are to be stabled. Although many owners prefer to bed on straw due to the reduced cost and relative ease of disposal, bedding on shavings (or similar low-dust material) can help reduce the inhaled dust in a horse’s environment and should be used in horses with lower airway inflammation.
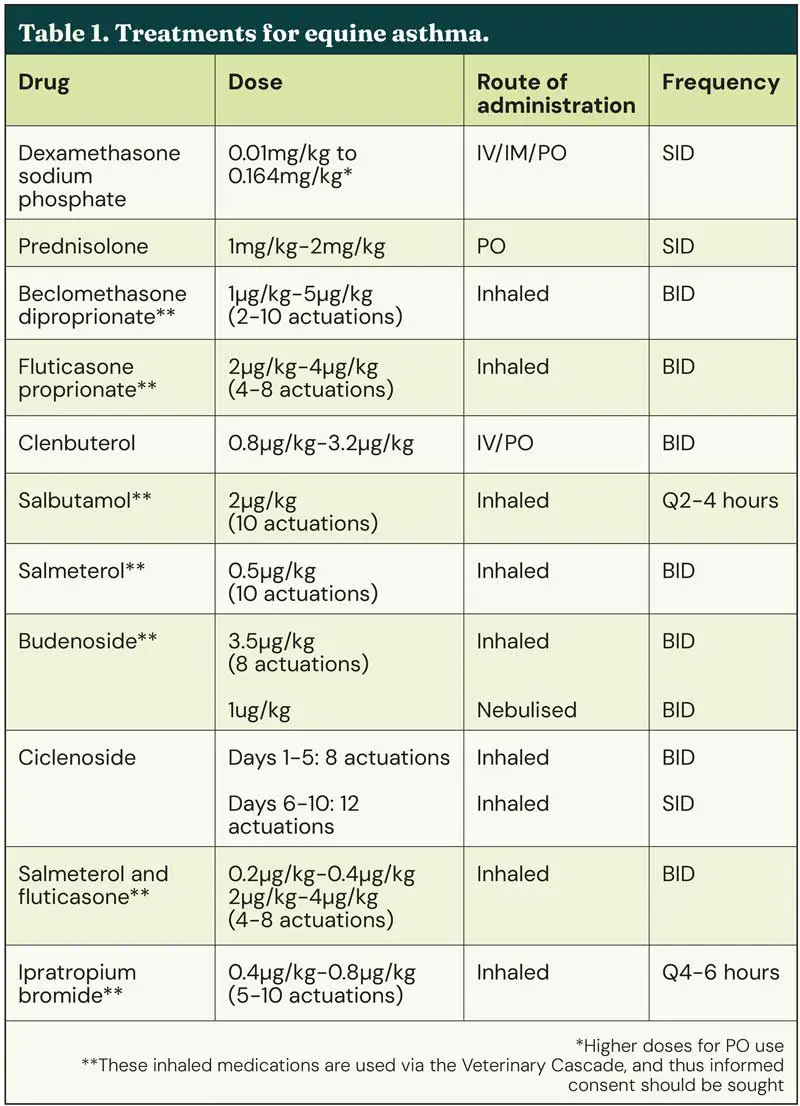
Treatments for EA are listed in Table 1.
In horses when environmental management is not sufficient to result in clinical improvement or in horses during acute exacerbations of sEA, corticosteroids (systemic or inhaled) are effective in improving airway function and relieving clinical signs. In human medicine, inhaled bronchodilators combined with systemic steroids are typically given to patients presented to emergency departments with severe asthma exacerbations14. A meta-analysis comparing the effectiveness of systemic versus inhaled corticosteroids in horses with sEA showed similar efficacy in improving clinical signs and lung function between the two routes of administration15.
In practice, it is often more effective in the author’s experience to use systemic medications in an acute exacerbation, especially if a horse has not been “trained” to accept the delivery device for the inhaled medications. IM or IV dexamethasone results in rapid (within three days) improvement in lung function, even when horses are kept indoors without measures to reduce dust16. A starting dose of 0.05mg/kg IM or IV is often used, and when this dose was used for seven days, lung function returned to normal (pasture) levels even when no management changes to minimise dust exposure were implemented17.
Oral prednisolone, which is licensed for use in asthmatic horses at a dose of 1mg/kg PO SID, does not appear to be as effective as dexamethasone. In one study, oral prednisolone (at a higher than label dose of 2mg/kg) was shown to have some efficacy at improving lung function of horses with severe asthma, even when kept indoors, but was not found to be as effective as PO dexamethasone. (0.05mg/kg)17 Oral dexamethasone (used in an off-label manner) has been shown in several studies to be effective at doses as low as 0.01mg/kg18,19. When using steroids orally, it is important to remember that the bioavailability is significantly reduced by feeding. In experimental studies, the oral steroids are given on an empty stomach and the horse then not fed for up to 60 minutes20.
Inhaled medications can be delivered via meter dose inhalers, via soft mist inhalers or via nebulisation. Owners often find nebulisation easier to perform than use of other devices that require contact with the nostril and ensuring the whole dose is inhaled.
Ciclesonide is the only licensed inhaled steroid available in the UK for horses. Ciclesonide is a prodrug that is metabolised in the lung epithelium following inhalation, resulting in a 100-fold increase in potency21. In a large (n=244) randomised controlled and blinded field study using clinical score to test the efficacy of inhaled ciclesonide, a significantly higher response rate and improvement in clinical score was seen in treated horses versus controls21.
The drug does not cause adrenal suppression, suggesting minimal systemic activity that may make it an appropriate choice in asthmatic horses that may be considered at increased risk for steroid-associated laminitis. A recent prospective, randomised, double-blinded, placebo-controlled clinical study evaluated the effect of a 10-day treatment course of ciclesonide in a small number of racehorses with moderate equine asthma. Treatment with inhaled ciclesonide improved clinical signs and decreased BALF mastocytic inflammation without change in the environment, although an improvement in neutrophilic or eosinophilic asthma could not be proven22.
Other inhaled corticosteroids that have been used with success in horses with asthma include fluticasone, beclomethasone and budesonide23,24. The inhaled medications must be administered using commercially available devices that incorporate a spacer and are placed either over one nostril or fitted as a face mask over both nostrils. Nebulisation of medications is an alternate method of delivering drugs in asthmatic horses. In two studies, nebulised dexamethasone (5mg SID for seven days; using two different types of nebulisers), however, did not result in a significant improvement in clinical score or pulmonary function tests in horses with sEA, despite improvements when the same (low) dose was given orally18,19. In both studies, systemic absorption (based on cortisol suppression) was identified. As such, treatment at this dose cannot be recommended for the treatment of horses with exacerbations of sEA, despite anecdotal reports that some horses respond to treatment.
Increasing the dose nebulised may improve efficacy, but would also presumably increase systemic absorption, negating a key perceived benefit of inhaled medications. Other nebulised medications, including lidocaine and budesonide (another steroid), have been investigated and may prove beneficial in the future. A study comparing the efficacy of nebulised lidocaine (1mg/kg BID) versus nebulised budesonide (1µg/kg BID) for 14 days in asthmatic horses showed an improvement in clinical score for both drugs, with lidocaine additionally resulting in a lower BALF neutrophil percentage and tracheal mucus score25.
Bronchodilators relax the airway and smooth muscles, providing symptomatic relief in asthmatic horses. Two classes exist – anti-cholinergics and β2 adrenergic agonists and they can be administered either as systemic or inhaled medications. Evidence is limited to suggest the superiority of either route for affected horses
In acute exacerbations accompanied by significant increases in respiratory rate and effort, systemic bronchodilators (using atropine, N butylscopolamine or clenbuterol) can provide immediate, albeit temporary, relief. Longer term, bronchodilators should not be used as a standalone treatment as they have no anti-inflammatory activity and tolerance or tachyphylaxis (desensitisation) occurs after 14 to 21 days of treatment26.
Clenbuterol has a dose-dependent effect, with a label dose rate of 0.8µg/kg-3.2µg/kg BID PO useful to help bronchodilate in the short term while environmental modifications are implemented, especially in horses not treated with corticosteroids. Not all horses respond to the drug, with an effect only seen in 75% of horses at the highest recommended dose of 3.2µg/kg and only 24% at the lowest dose27.
Inhaled bronchodilators can have a rapid effect (within 5 minutes). Short-acting medications such as albuterol/salbutamol last up to three hours, with longer-acting drugs such as salmeterol having a beneficial effect for up to 12 hours. Ipratropium is the only inhaled muscarinic cholinergic antagonist available that is commonly used in horses. Although there appears to be a large variation between horses, the typical duration of action is between four to six hours, with onset of action within 60 minutes.
The efficacy of treatment should be assessed by clinical evaluation and potentially repeat sampling of BALF. To ensure both the initial response and the longer-term management are optimal, re-examinations are best planned and scheduled in advance rather than relying on an owner to call if there is a problem.
No timings for these re-examinations are recommended, but in experimental studies, improvements in airway function and clinical score typically occur within 3 to 5 days of starting treatment with corticosteroids, so an initial examination 7 to 10 days into treatment would seem appropriate. At this time, if the horse is responding well to treatment (and environmental changes), evidence of respiratory disease should be significantly improved.
Repeat airway sampling is not recommended at this point, as evidence of inflammation will persist despite treatment (and clinical improvement) especially if no changes have been made to the environment. Repeat airway sampling may best be reserved for after the resolution of the “crisis”, when the horse has clinically improved to the extent that there are no (or very mild) clinical signs of respiratory disease and after environmental modifications have been optimised for at least six to eight weeks.
At this time a persistence of airway neutrophilia (especially BALF) would tend to suggest that the horse has ongoing dust exposure. If the environment has been optimised to the owner’s best ability, then these horses may benefit from longer-term inhaled corticosteroids, in particular, to minimise airway remodelling. Airway remodelling, which occurs in large part due to an increase in airway smooth muscle, is a major contributor to airway narrowing and obstruction with sEA-affected horses having three times more smooth muscle in their airways than age matched controls. Several studies have investigated the potential reversibility of this remodelling28,29.
Strict antigen avoidance (horses kept at pasture and fed no hay or haylage) resulted in a 30% decrease in airway smooth muscle across a 12-month period, with a similar result seen in horses treated with inhaled fluticasone for 12 weeks30. No significant immune suppression was observed in horses treated with fluticasone for longer than six months, and importantly, the antibody response after vaccination was not affected, suggesting that long-term treatment is associated with few, if any, side effects3. These studies highlight the importance of long-term management and follow up to help maintain optimal airway health in horses with sEA.
In horses with sEA that are overweight, weight loss may both help improve asthma symptoms and potentially reduce the risk of corticosteroid-associated laminitis.
In humans, obesity has an inverse relationship with residual lung volume and can exacerbate dyspnoea. Whether the same is true for horses is unknown, but improving weight can improve exercise tolerance and can only be beneficial to overall health.
Exercise is typically recommended to improve outcomes in people with asthma – exercise training reduces the risk of asthma exacerbations, improves exercise capacity and decreases the frequency and severity of flare ups31.
Encouraging exercise in horses with sEA once the worst symptoms are controlled should likewise be part of the holistic approach to management.
A recent study confirmed the positive impact of moderate exercise in horses with asthma. In this study, horses with sEA were either exercised (25 minutes of walking and trotting on the lunge) or turned out in a field for 25 minutes. Bronchodilation was measured before and after either exercise or turnout, and then again five minutes after salbutamol in the turnout group. Exercise, but not turnout, resulted in bronchodilation, which was equivalent to that achieved following salbutamol treatment32.
Considering the challenges owners often face in improving their horse’s environment and the limitations in using medications, especially in competing horses, a “drug-free” supplement that could aid in prevention or treatment of asthma would be beneficial.
Omega-3 fatty acids have an anti-inflammatory effect via a number of different mechanisms including reduction of substrates for pro-inflammatory mediators and reduction in the generation of inflammatory cytokines33. In one study, asthmatic horses were fed either with a supplement containing high concentrations of omega-3 fatty acids for eight weeks or placebo33. Both groups had similar changes to their environment (no hay and fed pelleted feed). As expected with the environmental changes, both groups showed an improvement in the clinical signs, but the magnitude of the response was greater in the supplemented horses. Additionally, supplemented horses showed significant improvements in their lung function and BALF neutrophilia, which was not seen in the placebo group33.
A second study investigated the impact of supplementing either fish oil (high in omega-3 fatty acids) or corn oil for four weeks in 55 racehorses fed a conventional diet (which included hay). BALF neutrophil percentage was significantly lower at the end of the four weeks in horses supplemented with fish oil but not corn oil, suggesting that increasing omega-3 fatty acids in the diet may help mitigate neutrophilic asthma in horses34.
Ongoing monitoring of clinical signs may help prevent a respiratory crisis by identifying worsening of symptoms before they become severe. A number of clinical scores that owners can utilise have been developed, and keeping a “respiratory diary” may be helpful to identify any possible triggers or trends.

Although the diagnosis of sEA is usually relatively easily obtained in affected horses diagnosis in horses with milder forms of the disease, in particular those showing only “poor performance”, can be challenging. Treatment is aimed at reducing inflammation and resultant bronchoconstriction, with environmental modifications to minimise inhalation of organic dust the key to disease management long term.
Despite well-characterised treatments that work well in experimental settings, not all horses will respond as well as we would like. In many instances, this is because environmental changes to minimise dust cannot be optimised, or medications cannot be administered due to other health issues or due to competition schedules. Ongoing research to explore competition legal therapies, to investigate other methods of diagnosing the condition and to identify possible biomarkers that could be used to “individualise” therapy is needed and will hopefully benefit asthmatic horses in the future.
Imogen Johns graduated from the University of Sydney in 1997 and then spent three years in private practice in Australia. She completed a residency in large animal internal medicine at the University of Pennsylvania between 2001 and 2003, became a diplomate of the American College of Veterinary Internal Medicine in 2004 and remained at the University of Pennsylvania as a lecturer until 2007. From 2007 until 2017, Imogen was employed as a senior lecturer in equine medicine at the RVC. She now works as an equine medicine specialist at B and W Equine Hospital in Gloucestershire.