24 Feb 2026
Victoria Colgate MA, VetMB, MSc, MRCVS and Richard Payne BSc, BVSc, CertES(Orth), DipECVS, MRCVS outline general considerations and principles for dealing with these emergency call scenarios

Image: Reimar / Adobe Stock
Wounds represent a common reason for an emergency call to the equine ambulatory vet, and fractures are also of significance – being commonplace in certain populations or, alternatively, being a rare but dramatic event where correct initial first aid can make all the difference.
Playing out in emotionally charged environments with an anxious horse and a highly stressed owner, it is important for the clinician to have a mental, and physical, toolkit at hand to ensure the best possible immediate care.
This article aims to give a general, rather than comprehensive, overview and highlight some important areas for consideration.
With both injuries, initial first aid treatment should progress through:
Universal to both scenarios is the need to obtain a detailed history and perform a general clinical examination. A recent history can be revealing in terms of the likely trauma sustained during injury occurrence and predispositions associated with certain signalments or work disciplines, and can be influential to your differential diagnoses.
It can be tempting to focus on what is often the clearly affected area, but for both wounds and fractures, potential for systemic compromise, haemorrhage, hypovolaemic shock and multiple trauma injuries makes a cursory clinical examination vital. Following initial examination, appropriate analgesia and sedation to relieve a horse’s pain and anxiety is a suitable first line of defence. As these injuries may have occurred during exercise, especially for fractures in the racehorse, it is important to consider that horses exercising hard may need up to twice the normal sedative dose to achieve an effect (Wright, 2017a). Once systemically stable, attention can be given to the specific injury.
Although an accurate diagnosis, and hence prognosis, can often not initially be achieved in these scenarios, effective communication is imperative and the responsibility of the clinician. It can be invaluable to have a good rapport with experts at a local referral hospital; advice regarding case-specific appropriate initial care and splinting for transport can greatly facilitate future management and contribute to overall outcome.
Equally, knowing when treatment is futile can manage owner expectations and protect horse welfare by ensuring long transportation is not undertaken when the prognosis is hopeless. In the other direction, effective client communication must be achieved in a pressurised environment. It can seem an insensitive topic to discuss, but consideration of finances, likely timeframe for repair and career goals for the horse are best considered once initial stabilisation and assessment has been made – but prior to embarking on a restorative treatment journey.
Fractures in the horse can usually be split into two aetiologies: those of a predictable configuration occurring most commonly in racehorses due to repetitive loading and resulting bone fatigue injury, and those occurring spontaneously due to trauma and one-off bone overload.
In either case, a horse suffering from a fracture will usually be extremely distressed, but this anxiety arises from limb instability, rather than the perception of pain (Wright, 2017b).
This is often demonstrated by repeated “lifting and placing” of the limb (Wright, 2017b) as the horse attempts to bear weight on an incomplete or unstable bony column. As well as being distressing for the horse, this activity is also highly damaging to the fracture margins (Wright, 2017b) and overlying soft tissue; eburnation of bone ends and potential progression to open fracture by bony penetration of the horses’ thin skin, could compromise repair and cause progression to fatal injury. Accordingly, fracture stabilisation via splinting is the primary first aid consideration in these cases.
Overall, the goals of splinting are to:
Some specifics will be explored later, but the mainstay of immobilisation has been through the use of a Robert Jones Bandage (RJB) with/without external splints. Recently, bandage casts have become more commonplace and offer more reliable 360° support for the distal limb.

To be prepared for all emergency scenarios, it would be sensible to always carry enough bandage material for a full-limb RJB, and ideally some splints of various sizes, in the car. A note of caution is that a badly applied splint can do more harm than good, creating a moment arm at the fracture site and increasing soft tissue damage (Morgan and Galuppo, 2021).
As appropriate splinting technique is dependent on fracture location, where location cannot be determined but fracture is suspected, support and splinting should not be used (Wright, 2017b).
Appropriate splinting is particularly important if transportation to a referral facility is to be considered. Additional forces during motion, and the anxiety associated with weight bearing on three legs for the journey, can otherwise lead to fracture deterioration and reduce the chance of successful surgical repair.
As it is easier to control acceleration than braking, it has been suggested that horses with forelimb fractures should travel backwards, and those with hindlimb fractures forward (Morgan and Galuppo, 2021; Mudge and Bramlage, 2007). If possible, a specialised trailer should be used, but of most importance is safe, calm and expedient travel to a place of further treatment or safety. It is actually unloading and loading, rather than the distance of travel, that are most crucial to a successful journey (Wright, 2017b) and a trailer with a shallow ramp angle is preferred.
NSAIDS with appropriate limb support and immobilisation should provide all the analgesia necessary to achieve acceptable comfort for transport (Wright, 2017a).
As far as is possible, it is important to elucidate fracture location, configuration and severity prior to splint application. The forces to be neutralised are dependent on anatomical location of the fracture and, as such, best splinting technique is region dependent (Morgan and Galuppo, 2021).
Many excellent resources (Mudge and Bramlage, 2007; Wright, 2017b; Wright 2017c; Morgan and Galuppo, 2021) are available to give general regional based advice for appropriate fracture support, but there is no universally sound principle and every fracture should be individually evaluated. The aforementioned resources should be consulted for greater detail, but some general principles are outlined in Table 1.
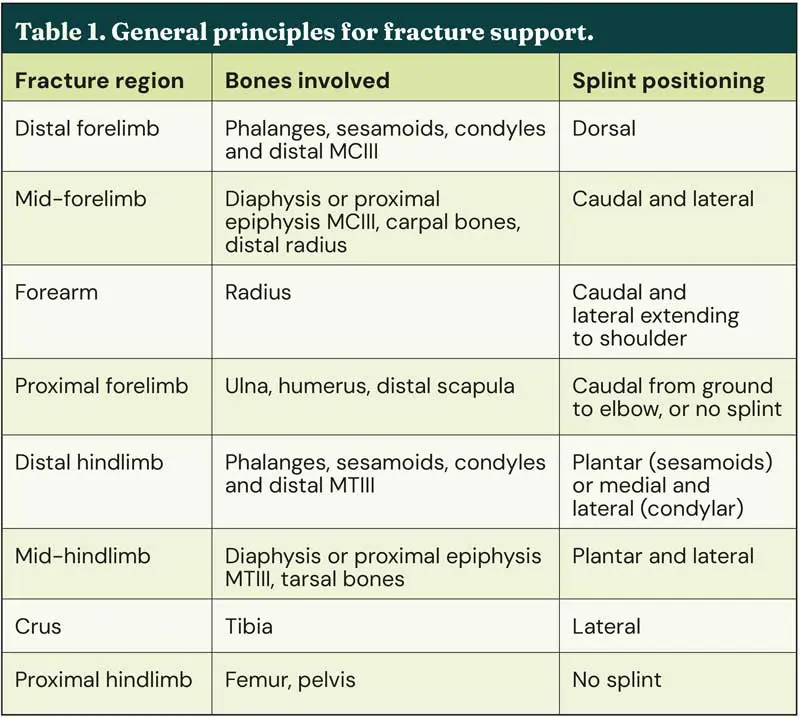
In the distal forelimb, or hindlimb, fracture of the sesamoids, phalanges or metacarpal/metatarsal (MC/MT) III condyles leads to loss of the intact bony column and tension on the palmar/plantar soft tissues. These are common racehorse injuries eminently suited to successful surgical repair, as long as further displacement does not occur – making appropriate first aid splinting crucial to outcome. In particular, any fractures with increased potential for propagation, such as medial condylar fractures that tend to spiral proximally, should be promptly and rigidly immobilised. However, sesamoid and phalangeal, versus condylar, fractures require different methods of stabilisation.
Sesamoid and phalangeal fractures are best immobilised with the distal limb in flexion, thus aligning the dorsal cortices of the bones, or by rigid support with the limb in a neutral position. Many splints are commercially available, such as the Kimzey Leg Saver Splint, that provide fast and convenient stabilisation. The Kimzey splint is used on racecourses worldwide, but it must be remembered that it provides no mediolateral stability (Wright, 2017b), and accordingly, is not suited to stabilisation of condylar fractures, which require immobilisation in extension, in the normal weight-bearing position (Wright, 2017c).
Since 2022, all British racecourses have been equipped with a fracture support system (Wright, 2022) to allow easy access to all that should be needed to stabilise a racecourse fracture. Included in this system is the Newmarket Compression Boot, which, capable of maintaining fetlock angle at 150°, has taken over as the ideal temporary immobilisation method for condylar and phalangeal fractures (Wright, 2022).
But commercial splints are rarely tolerated in the hindlimbs, where the reciprocal apparatus dictates the need for a different splinting technique to that used in the distal forelimb. In the hindlimb, fewer bandage layers should generally be placed, but a RJB with medial and lateral splints is generally the stabilisation method of choice. In the case of forelimb, or hindlimb, biaxial sesamoid fractures attention must be given to integrity of the neurovascular bundle. This injury causes complete fetlock collapse, with stretching to, and potential damage of, the neurovascular bundle and without effective maintenance of blood supply, attempts at repair are futile.
Fractures of the mid or proximal radius require specific consideration due to two factors. When the radius no longer forms a single intact bone, it causes both the laterally placed forearm flexor and extensor muscles to act as abductors (Mudge and Bramlage, 2007; Wright 2017c). This lateral pull increases the risk of development of an open fracture as sharp bone ends could pierce through the thin medial skin, and makes timely stabilisation via application of a lateral splint to the level of the shoulder imperative (Mudge and Bramlage, 2007).
The ulna, although part of the forearm, is best grouped with the humerus and scapula (proximal forelimb) when it comes to splinting, and here the most important consideration is the loss of triceps function that will render the horse unable to fix the carpus in extension. In general, immobilisation of proximal forelimb fractures is contraindicated, but a caudal splint from elbow to ground should be considered to counteract the loss of triceps function and fix the carpus in extension to allow weight-bearing (Morgan and Galuppo, 2021).
The approach should always be “do no harm” and it is important to remember that for some fractures, immobilisation and splinting is either simply not possible, not necessary, or contra-indicated. Often this applies to fractures of the more proximal limb, such as the humerus, scapula, femur and pelvis. Here, although direct fracture immobilisation should not be attempted, application of a distal limb support bandage can provide counter pressure to minimise swelling and reduce associated discomfort (Wright, 2017c).
Equally, carpal bone fractures are rarely associated with instability, and thus do not require splinting, but a presage bandage can minimise swelling (Georgetti, 2022).
Wound management makes up a notable proportion of equine clinical practice and, on top of this, due to their flight or fight nature and living environment, horses are predisposed to contaminated wounds with significant secondary trauma.
Perhaps the most important aspect to remember in initial assessment of equine wounds is that huge traumatic wounds can often heal without complication, while the seemingly innocent tiny puncture wound can be life-threatening due to synovial sepsis.
With initial wound debridement and care having the greatest impact on overall healing (Eggleston, 2018a), clinicians are best placed to have a significant influence on the process, and yet, a lot of equine wounds are initially managed by owners without veterinary consultation (Theoret et al, 2016; Zambroni et al, 2025). This means that acute veterinary management of wounds can actually start with a chronic process.
To have a positive impact on wound healing requires an excellent knowledge of anatomy and the stages of wound healing, as well as following a detailed wound-specific, and general, examination. As with the fracture case, initial gross evaluation of the patient is important to determine any signs of systemic compromise or underlying disease, and a full body examination crucial to ensure any small secondary wounds are not overlooked.
Long-standing conditions, such as pituitary pars intermedia dysfunction, are immunosuppressive and can cause significant delays and complications to the healing process – being prepared equalling being forewarned.
Wound healing is a three-stage biological process that sees progression through acute inflammation and debridement, to proliferation, and finally to maturation and remodelling. Through interventions, the aim is to ensure acute inflammation rapidly progresses to the proliferative repair phase without the development of chronic inflammation (Knottenbelt, 1997), which heralds delayed wound healing, with potential development of exuberant granulation tissue (EGT) and scarring.
Initial evaluation should incorporate careful clipping of the hair – starting close to the wound and moving outwards (Frees, 2018) – after application of a water-based lubricant to minimise additional wound contamination with hair. Clipping allows better visualisation of the affected area and should be followed by wound lavage under an appropriate pressure (around 8 to 15 psi) and at an oblique angle (Frees, 2018). This can normally easily be achieved using a 19G needle and 35ml syringe (Eggleston, 2018a).
Traditionally, the advice has always been to use sterile isotonic fluids for wound lavage, but following human evidence summarised in the BEVA Primary Care Guidelines on wound management, tap water could be considered (Freeman et al, 2021). The use of antiseptics, such as povidone iodine or chlorohexidine, in addition to lavage fluids, is common, but evidence for use is actually more debatable. Indeed, these antiseptics are cytotoxic and must be used at an appropriate concentration, but such a concentration has not been scientifically elucidated (Freeman et al, 2021). Proper cleaning and debridement are essential wound bed preparations prior to closure due to the contaminated nature of equine wounds. Although contamination does not equal infection, infection is likely to develop when there are greater than 106 bacteria per gram of tissue (Frees, 2018).
Wounds are best evaluated in light of the deepest tissue structure affected (Gaughan, 2018). Therefore, after suitable cleaning and debridement, visual examination, manipulation and exploration with a gloved finger or sterile metal probe is prudent. An important factor to determine is the potential for communication with a synovial structure and here it should be remembered that if the wound occurred with the limb in a different anatomical position, now examining the stationary horse it may not obviously be over a joint. Synovial communication is best determined by sterile distension of the suspect joint and observation for fluid egress from the wound; confirming a connection.
Following thorough cleaning and evaluation, and ruling out of referral, acute wound management then extends to decisions on closure method and management going forward. Primary closure offers the best chance of a functional and cosmetic reconstruction of the affected tissue, but is unsuitable in some instances, most notably, where you have significant contamination, a poor bloody supply or excessive tension (Kamus and Theoret, 2018).
Delayed primary closure can be used for wounds that could be sutured but currently are heavily contaminated. The one-to-three day time interval allows for better preparation of the wound bed to increase the chance of successful primary healing (Kamus and Theoret, 2018).
Second-intention healing is where there is no attempt to oppose the wound edges and the wound is left to primarily heal by granulation and epithelisation, rather than contraction (Kamus and Theoret, 2018).
This can be the best, and sometimes only, option in areas of high movement or wounds with extensive skin loss and tension, and heavy contamination. However, it should be remembered that wounds left to heal by this method often lead to greater scarring and weakness, and it is not necessarily a cheaper option. Costs of repeated bandage changes and wound debridement to deal with EGT can often exceed those of initial primary closure via suturing. Finally, delayed secondary closure can also be an option. Here, if a healthy granulation bed forms after initial management via second intention healing, it can then be appropriate to suture the wound edges in an attempt to increase rapidity of healing and prevent further development of EGT (Kamus and Theoret, 2018).
As our equine patients cannot be effectively immobilised or placed in a clean environment, good bandaging is key to equine wound management (Eggleston, 2018b). Bandages can have a positive impact on healing through assisting with haemostasis, protecting from further trauma, contamination and desiccation, and restricting movement. However, as with fracture immobilisation, the keyword here is “good” and appropriate bandage care often requires a substantial time and money investment from the owner.
Considerations of specific wound types
A notable difference between horses and ponies has been identified in terms of propensity for effective wound healing. Ponies are thought to be less susceptible to the complications of dehiscence, EGT and bone sequestration (Kamus and Theoret, 2018) as effective wound healing is initiated by a fast and efficient acute inflammatory phase (Eggleston, 2018a). In contrast, in the horse, a weak initial inflammatory response leads to persistent fibroplasia, poor wound contraction and development of chronic inflammation with increased chance of EGT (Eggleston, 2018a).
A similar consideration should be given to wounds on the trunk, versus those on the distal limb. Wounds on the trunk, except for those on the dorsum that have compromised drainage and are easily secondarily infected (Eggleston, 2018a), generally heal rapidly and without complication. This is due to the abundance of underlying soft tissue and ability of the wound to proceed with effective contraction (Knottenbelt, 1997; Eggleston, 2018a). In contrast, distal limb wounds show limited contraction (Knottenbelt, 1997) and chronic inflammation, which leads to increased wound retraction, epithelisation and increased production of EGT (Eggleston, 2018a).
Additionally, the lack of soft tissue protection means greater potential for injury to important underlying tendons, ligaments and neurovascular structures. A wound resulting in laceration to the flexor tendons equates to a severe injury that needs careful management through emergency splinting and referral to a hospital facility if athletic ability is to be maintained. However, the dorsally located extensor tendons can be badly damaged without adversely affecting prognosis. A supportive bandage or splint may be necessary to prevent knuckling over, though, and healing often delayed due to increased motion at the wound site (Caston, 2012).
To heal effectively, wounds must be stabilised, be free of infection, and have an effective blood supply. Accordingly, it is important to resist the temptation of trying to suture wounds that will almost certainly break down due to absence of one or more of these factors. For example, an upward pointing flap wound on the back of the fetlock, and an extensive axilla wound, are unlikely to respond positively to primary closure due to poor blood supply, and excessive movement and dead space, respectively. Such wounds are best managed through second intention healing from the outset.
A final worthy note is with regard to thoracic wounds. Often these are of no additional significance beyond routine wound care, but the potential for thoracic cavity penetration should always be considered. Penetration will allow gas to enter the pleural cavity, leading to pneumothorax and lung collapse. In these cases, an attempt to re-establish an airtight cavity should be made through use of an Ioban drape or cling film wrapped around the chest, prior to immediate referral (Sprayberry and Barrett, 2015). Also, remember that due to the horse’s incomplete mediastinum, a unilateral penetration can lead to bilateral pneumothorax (Sprayberry and Barrett, 2015).
There can be challenges to performing immediate critical care to the fracture or wound patient, but calm communication, relief of pain and anxiety in the horse – and following a simple decision toolkit –can lead to guided decision-making and the best outcome for horse and owner alike.
Victoria Colgate qualified from the University of Cambridge in 2014, and then completed a clinical training scholarship at its equine hospital before working in a busy polo practice in Ascot. She joined Rossdales Equine Hospital in June 2017 as the Margaret Giffen Resident in Clinical Research, where in addition to carrying out research projects she attained an MSc in Veterinary Epidemiology and Public Health. After time away in a specialist role as a veterinary epidemiologist at Equine Infectious Disease Surveillance (EIDS), Vicky returned to Rossdales in July 2023 as a research associate, a role funded by the Margaret Giffen Charitable Trust.
Richard Payne is the clinical director responsible for Rossdales Equine Hospital and is one of the busiest equine surgeons in the UK. He graduated from the University of Bristol in 1995, having also obtained a degree in pharmacology. After a year in mixed practice, he moved to Rossdales where he completed a three year residency in equine surgery. He became a partner in 2002 and a clinical director in 2021. He has a large and varied caseload of elective and emergency surgery, with a special interest in standing and minimally invasive surgery, including arthroscopy, fracture repair, laparoscopy and laser surgery.