24 Feb 2026
Canine chronic inflammatory enteropathies: diagnostic approach
Ferran Valls Sanchez DVM, DipECVIM‑CA, MRCVS explains the updated classification of, and process for diagnosing, these gastrointestinal disorders in dogs.
Ferran Valls Sanchez
Job Title
Image: adogslifephoto / Adobe Stock
I wrote this article a few days before the end of last year – a time for social media wrap-ups and lists of goals and wishes. I want to go to Egypt in 2026, and while you are reading this, your mind has inevitably conjured an image of a pyramid.
Today, we will use a pyramid as a framework for this article1,2, albeit, a different one (Figure 1).
On the left side of Figure 1, you can see how chronic inflammatory enteropathies (CIE) were previously classified, and on the right, the updated classification.
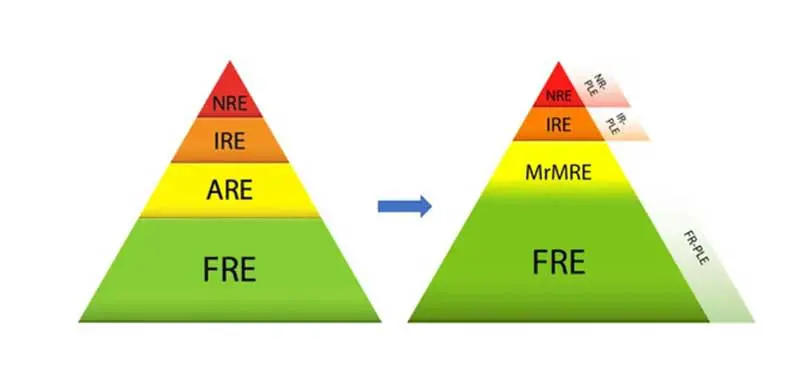
When we suspect that a patient may suffer from CIE, remembering this image is extremely useful, as it reflects which type of CIE is more common.
In addition, it illustrates the pathway to reach a diagnosis: if we understand the pyramid as an arrowhead, it shows in order what to rule out or rule in first, then second, and so on.
CIEs: what are they, and when should we think about them?
CIEs are inflammatory conditions (with histological evidence) of the gastrointestinal tract, characterised by chronic or recurrent gastrointestinal signs such as vomiting, diarrhoea, abdominal pain, nausea, weight loss, or a combination of these. This disease is multifactorial in origin, involving genetics, diet, microbiota and immune system factors2.
Chronic vomiting and diarrhoea are common clinical complaints, and CIE should always be considered when establishing a list of differential diagnoses for these signs. This is particularly true in older dogs, where infectious causes are less likely and CIE and neoplasia are often at the top of the list.
CIEs are classified into food-responsive enteropathy (FRE), microbiota-related modification-responsive enteropathy (MrMRE), immunosuppressant-responsive enteropathy (IRE) and non-responsive enteropathy (NRE). However, I prefer to refer to the last two as inflammatory bowel disease (IBD).
All of these subtypes can lead to a syndrome called protein-losing enteropathy (PLE), in which protein leakage and malabsorption result in severe hypoalbuminaemia. This represents a more severe clinical scenario and should raise greater concern. PLEs are more commonly associated with IBD, but some PLE cases respond exclusively to dietary management, meaning that FRE can also cause PLE.
From bottom to top
You say food-responsive; I say diet trials
FRE is diagnosed when gastrointestinal signs resolve or significantly improve within two weeks of starting a diet trial.
FRE is the most common type of CIE, accounting for more than 50% of cases. These dogs are often younger and present with milder clinical signs. Hydrolysed diets or novel protein diets (homemade or commercial) are usually among the first choices. It is important to raise awareness of the relevance of dietary management as a first-line treatment in CIE. In one study, two-thirds of cases initially considered non-responsive to diet responded to a different diet trial, and many treatment-naive cases improved with exclusive dietary management3. Another research group reported similar findings, with 19 out of 24 dogs reclassified from NRE to FRE over a one-year period4.
Setting expectations regarding the number of diet trials a dog (or cat) may require during initial consultations is fundamental. Unpublished data suggest that some patients may need up to eight diet trials before finding an effective one. In my opinion, acceptance of multiple diet trials is higher when this is discussed at the first consultation.
A thorough dietary history should be obtained to understand which diets have been used previously and how they were administered, including owner compliance. Sometimes, I ask pet parents to write down a list of diets used (type, duration, whether other foods were given, and whether any clinical improvement was observed).
Finally, if the dog is reluctant to eat the recommended diets, referral to a nutrition specialist should be offered, as they can formulate a homemade diet tailored to palatability.
You say MrMRE; I say probiotics and FMT
In recent years, there has been extensive research on the gut microbiota, with growing evidence supporting the use of probiotics and faecal microbiota transplantation (FMT). Alterations in gut microbiota composition and function (dysbiosis) are associated with canine CIEs1.
As shown in the updated pyramid compared with the older version (Figure 1), there is now a recognised group of cases that respond to microbiota-related interventions. Antibiotic-responsive enteropathy has been removed from the classification.
In dogs with CIE refractory to dietary management, FMT has been shown to improve clinical signs5. Dogs with milder clinical signs and absent or mild dysbiosis tend to respond better. Dysbiosis can be assessed using the dysbiosis index (DI). Another study suggested that FMT may also serve as an adjunctive treatment in dogs with CIE, with better responses again seen in dogs with lower DI values6.
FMT should be strongly considered when diet trials have failed, before moving on to immunosuppressive therapies. One of my earlier mistakes was using FMT as a “last resort” (for example, in severe PLE cases, where it predictably failed). Patient selection is, therefore, crucial to maximise success. In 2024, guidelines were published outlining appropriate FMT protocols7.
Regarding probiotics (live microorganisms), prebiotics (substrates for beneficial microorganisms) and synbiotics (combinations of both), the main conclusion is that further large-scale studies are needed. Some studies using an eight-strain lactic acid bacteria mixture and Saccharomyces boulardii have shown promising results2.
Finally, one publication reported clinical remission in two dogs with non-responsive IBD treated with colestyramine, a bile acid sequestrant8. The proposed mechanism is correction of excess primary bile acids resulting from bile salt dysmetabolism associated with intestinal dysbiosis.
You say IBD; I say let’s hope it responds to immunosuppressants
According to several studies, IREs account for approximately 10% to 25% of CIE cases1. Prednisolone is the most commonly used first-line treatment. If there are significant side effects or inadequate response, other drugs such as ciclosporin or chlorambucil may be added.
A thorough discussion of prednisolone side effects is essential, so that pet parents are informed and do not panic. This is also an opportunity to provide practical advice to improve quality of life for both the dog and the owner (for example, increased access to outdoor toileting, constant access to water, caution with leftovers and bins if scavenging develops, and avoiding ad libitum feeding).
As mentioned previously, a careful review of the clinical history and previous diet trials (to confirm that FRE has been adequately excluded) is fundamental before initiating immunosuppressive therapy.
Some cases do not respond to immunosuppressants and are associated with a poorer prognosis.
You said antibiotics; I say no
In the past, antibiotics such as metronidazole were commonly used in cases of chronic diarrhoea. However, over the past decade, evidence has emerged showing limited benefit and significant negative effects on gut microbiota9.
Persistent alterations in microbiota diversity have been reported following the use of metronidazole and tylosin, which may explain the high relapse rates observed after treatment discontinuation9.
Additionally, global concerns regarding antimicrobial resistance make antibiotic stewardship particularly important within the one health framework.
Comments on the diagnostic approach to chronic diarrhoea/vomiting – CIE
- Rule out infectious causes (for example, faecal testing) and non-gastrointestinal differentials such as endocrinopathies and pancreatitis (for example, biochemistry, basal cortisol, with or without canine pancreatic lipase immunoreactivity or trypsin-like immunoreactivity).
- Measure cobalamin (vitamin B12). This vitamin is absorbed in the ileum and if levels are decreased or at the low end of the reference range (less than 400ng/L), supplementation is recommended10 and may aid clinical resolution. Oral supplementation has been shown to be as effective as injectable therapy11.
- Discuss abdominal ultrasound. Although some studies question its utility when approaching chronic diarrhoea12, it can help assess suspicion for neoplasia and rule out non-gastrointestinal conditions such as chronic pancreatitis. While not perfect, ultrasound is accessible, widely used and, generally, affordable.
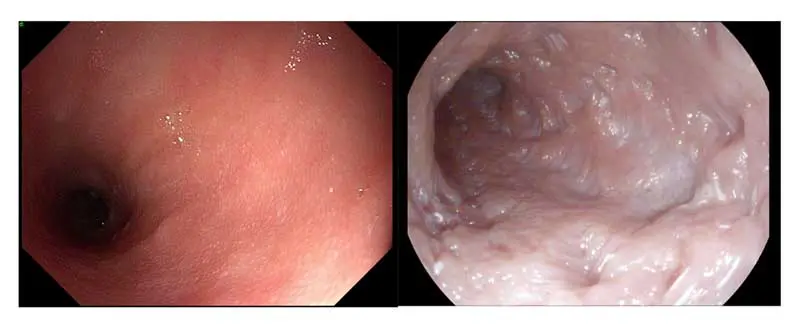
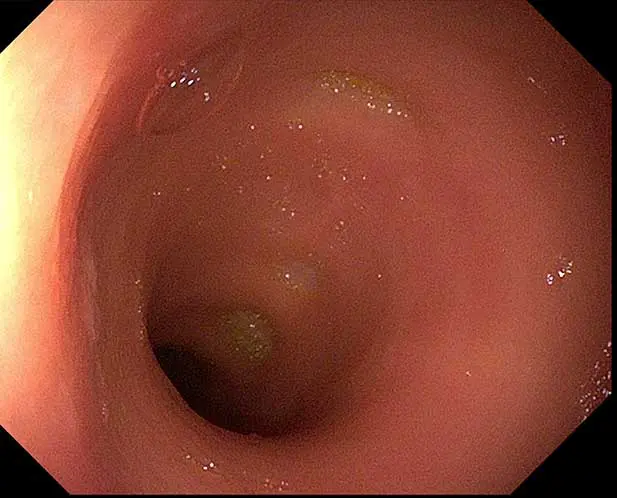
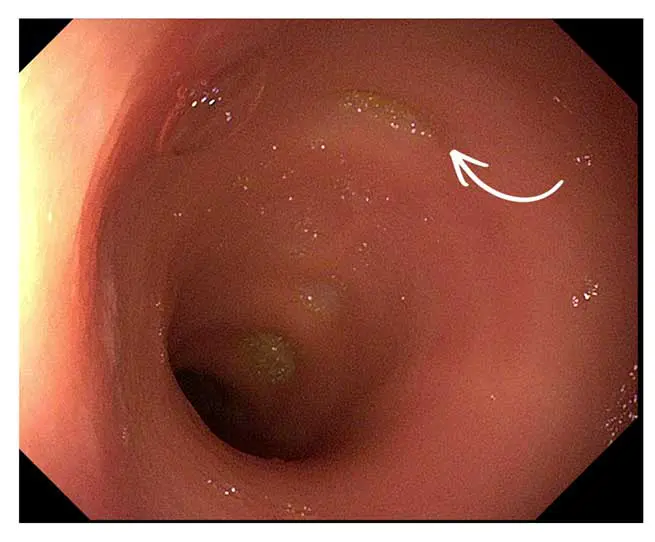
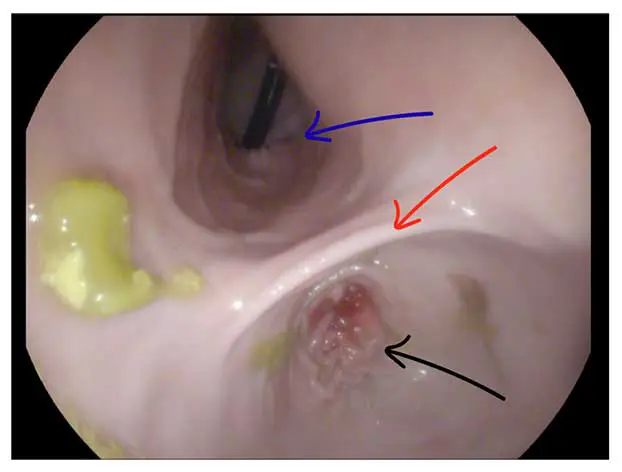
- Consider endoscopy (upper and/or lower). The decision should be guided by history (for example, additional clinical signs, severe weight loss, PLE), age, anaesthetic risk, owner expectations regarding exclusion of neoplasia and financial considerations (Figures 2-4).
- Perform multiple diet trials (with strict compliance), using hydrolysed or novel protein diets. If palatability is an issue, consider a homemade diet formulated by a nutritionist.
- Consider whether the patient may benefit from FMT; this is more likely to be effective in younger patients with milder signs and a low DI.
- Endoscopy (upper and/or lower) should be strongly discussed before initiating corticosteroid therapy if not already performed. Although endoscopy and histology are the gold standard, our recent study concluded that the risk of finding a neoplastic process was low in dogs with chronic diarrhoea and “boring” ultrasound13. This data is useful in cases where the anaesthetic risk is high or there are financial constraints to make an informed decision.
- Trial immunosuppressive therapy where indicated.
Take to clinic messages
- Remember the CIE pyramid: FRE is the most common subtype.
- Most cases improve or resolve with dietary management; persistence with diet trials is crucial.
- Gut microbiota research has expanded rapidly. FMT should be discussed when diet trials fail – particularly in younger dogs with low DI values.
- Prednisolone is usually the first-choice immunosuppressant, but others such as ciclosporin or chlorambucil may be required.
- Some IBD cases do not respond to immunosuppressive therapy and carry a poorer prognosis.
- As a general rule, antibiotics should be avoided.

- Use of some of the drugs in this article is under the veterinary medicine cascade.
- Article appeared in Vet Times (24 February 2026), Volume 56, Issue 8, Pages 6-8
Ferran Valls Sanchez graduated from the Autonomous University of Barcelona in 2011 and is a European specialist in small animal internal medicine and co-founder of WeYouVets, a veterinary startup dedicated to bringing specialist internal medicine support directly to first-opinion practices, alongside high-quality education. Ferran is passionate about making specialist knowledge practical, accessible and relevant to everyday clinical work. In 2025, he also co-founded VetCracks, an educational initiative for veterinarians in Latin America, built on the same values as WeYouVets and focused on accessible, high-quality, and people-centred veterinary education. Visit weyouvets.com
Similar content on vettimes.com
References
- 1. Dupouy-Manescau N, Méric T, Sénécat O et al (2024). Updating the classification of chronic inflammatory enteropathies in dogs, Animals 14(5): 681.
- 2. Jergens AE and Heilmann RM (2022). Canine chronic enteropathy – current state-of-the-art and emerging concepts, Frontiers in Veterinary Science 9: 923013.
- 3. Rodrigues SD, Mendoza B, Dias MJ et al (2025). Association of diet with treatment response in dogs with chronic enteropathy: a retrospective multicenter study, Journal of Veterinary Internal Medicine 39(3): e70071.
- 4. Hodel S, Brugger D and Kook PH (2024). Long-term evaluation of the initial response to therapy in 60 dogs with chronic inflammatory enteropathy, Journal of Veterinary Internal Medicine 38(5): 2,444-2,453.
- 5. Vecchiato CG, Sabetti MC, Sung CH et al (2025). Effect of faecal microbial transplantation on clinical outcome, faecal microbiota and metabolome in dogs with chronic enteropathy refractory to diet, Scientific Reports 15(1): 11957.
- 6. Toresson L, Spillmann T, Pilla R et al (2023). Clinical effects of faecal microbiota transplantation as adjunctive therapy in dogs with chronic enteropathies – a retrospective case series of 41 dogs, Veterinary Sciences 10(4): 271.
- 7. Winston JA, Suchodolski JS, Gaschen F et al (2024). Clinical guidelines for fecal microbiota transplantation in companion animals, Advances in Small Animal Care 5(1): 79-107.
- 8. Toresson L, Steiner JM and Suchodolski JS (2021). Cholestyramine treatment in two dogs with presumptive bile acid diarrhoea: a case report, Canine Genetics and Epidemiology 8(1): 1.
- 9. Cerquetella M, Rossi G, Suchodolski JS et al (2020). Proposal for rational antibacterial use in the diagnosis and treatment of dogs with chronic diarrhoea, Journal of Small Animal Practice 61(4): 211-215.
- 10. Texas A&M Gastrointestinal Laboratory. Cobalamin (vitamin B12) information, https://vetmed.tamu.edu/gilab/research/cobalamininformation
- 11. Toresson L, Steiner JM, Razdan P et al (2018). Comparison of efficacy of oral and parenteral cobalamin supplementation in normalising low cobalamin concentrations in dogs: a randomised controlled study, The Veterinary Journal 232: 27-32.
- 12. Leib MS, Larson MM, Grant DC et al (2012). Diagnostic utility of abdominal ultrasonography in dogs with chronic diarrhoea, Journal of Veterinary Internal Medicine 26(6): 1,288-1,294.
- 13. Jolly-Frahija I, Dormon S, Shing H and Sanchez FV (2025). Endoscopic biopsy assessment of neoplastic prevalence in dogs with chronic diarrhoea and non-suggestive ultrasound findings, Sci 7(2): 39.