Senior pets – considerations of medication use in cats and dogs
Mike Davies BVetMed, CertVR, CertSAO, FRCVS provides an overview of common conditions seen and medications used in older pets, including when and when not to screen first and monitor later.
Mike Davies
Job Title
Image: Alex Renko / Adobe Stock
Ageing changes occur in all tissues and are progressive, resulting in reduced tissue reserve. These changes may alter drug pharmacodynamics and pharmacokinetics.
Elderly patients are more likely to develop obesity, which alters drug distribution, safety and efficacy, and the elderly (especially cats) are also susceptible to develop sarcopenia with loss of lean body muscle mass, which also alters drug distribution.
Age-related diseases are more prevalent as animals reach the last third of expected lifespan and especially the final quartile.
Many of these diseases can be subclinical for a number of years before any clinical signs become evident.
Before administering drugs with narrow safety margins to a geriatric patient, the animal should be screened for the most common diseases, some of which may impact drug safety or efficacy.
Common age-related diseases in dogs include:
Endocardiosis (58% of dogs older than nine years).
Diabetes mellitus (1 out of 200 dogs).
Hypothyroidism.
Dental (95% by eight years).
Degenerative joint disease.
Prostatic disease.
Cushing’s syndrome.
Renal failure.
Liver disease (1 out of 53 PME).
Acute pancreatitis (1 out of 300).
Neoplasia.
Meanwhile, common age-related diseases in cats include:
Dental disease (85% of cats older than five years).
Obesity (25%).
Endocrine disease.
Diabetes mellitus (1 out of 400 cats).
Hyperthyroidism (1 out of 300 cats).
Acromegaly.
Renal disease (chronic, acute).
Feline triad syndrome.
Inflammatory bowel disease.
Pancreatitis (1 out of 666 cats).
Cholangitis/cholangiohepatitis.
Neoplasia.
Constipation.
Vestibular syndrome.
Ageing changes that impact on drug use
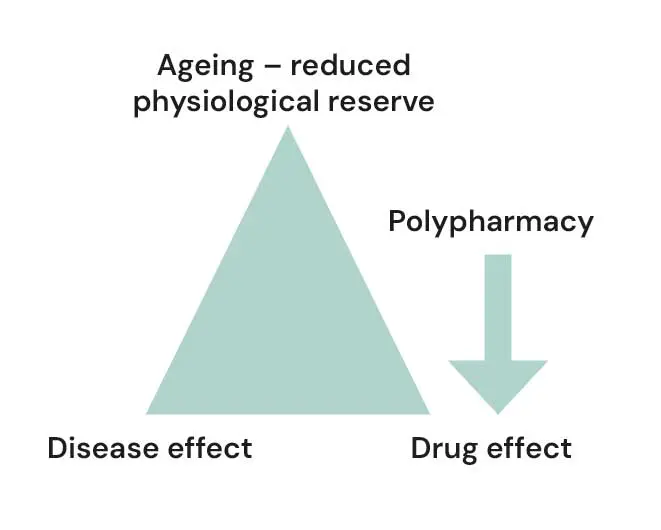
In elderly patients, it is important to consider the effects of ageing, age-related diseases and drug-drug interactions, all of which may affect safety and efficacy (Figure 1).
Figure 1. Basic considerations of ageing and therapeutics.
Drug absorption may be decreased, as functional small intestine surface area may reduce with age, but usually this is of little clinical significance. In some cases, the SPC of a drug will specify the timing of oral dosing with feeding; for example, the SPC of pimobendan states: “After oral administration of the product the absolute bioavailability is [60% to 63%]. Since simultaneous or previous food intake reduces the bioavailability, pimobendan should be administered about one hour before feeding.”
This advice is particularly important in elderly dogs and those with gastrointestinal disease such as inflammatory bowel disease.
Drug distribution may alter due to age-related body composition changes:
Reduced total body water increases concentration of drug in body fluids.
Reduced serum albumin increases free fraction of protein-bound drugs in plasmas.
Increased body fat increases concentrations of fatty acids in blood and prolongs elimination of fat-soluble drugs.
Four key considerations in drug administration exist:
Response of target organ to drug dose (pharmacodynamics).
Host’s ability to adapt to drug effects (homeostasis).
Ability of drug to reach target site (pharmacokinetics).
Host’s ability to eliminate drug.
Hepatic changes in ageing are likely to include:
Reduced liver mass.
Reduced hepatic blood flow.
Reduced first pass metabolism, causing decreased rate of biotransformation.
Some drugs are specifically contraindicated in the presence of liver disease; for example, according to the SPC: “Since pimobendan is metabolised mainly via the liver, it should not be used in dogs with severe impairment of liver function”.
Renal changes in ageing are likely to include:
Reduced renal blood flow.
Reduced glomerular filtration rate.
Reduced elimination rate.
Some drugs are specifically contraindicated if renal disease is present; for example, NSAIDs.
Older patients often require a reduction in drug dose, as they are more sensitive and less able to eliminate them, due to ageing changes and:
Presence of concurrent disease(s).
Presence of subclinical disease(s).
Concurrent therapeutic agents.
High therapeutic index of drug and severity of adverse effects.
For drugs with high therapeutic index and no significant adverse effects (such as penicillin, cephalosporins), start at the usual dose.
For drugs with low therapeutic index and significant adverse effects (for example, opioid analgesics, tranquillisers such as acepromazine [ACP], theophylline, aminoglycosides, anti-arrhythmic drugs, digoxin): if a safer alternative is available, use that first; if not, start at 33% to 50% of the usual dose or increase dose intervals.
If renal impairment is present, drug dose can be adjusted appropriately based on creatinine clearance rate (CCr):
0.5ml/min/kg to 1ml/min/kg: two-fold increase in dosing interval.
0.3ml/min/kg to 0.5ml/min/kg: three-fold increase in dosing interval.
0.3ml/min/kg: four-fold increase in dosing interval.
CCr can be estimated: 88.4/serum creatinine (µmol/L).
Or: use one-third usual dose if isosthenuric; one-quarter usual dose if azotaemic.
The meloxicam SPC (datasheet) for cats states: “Do not use in cats suffering from gastrointestinal disorders such as irritation and haemorrhage, impaired hepatic, cardiac or renal function and haemorrhagic disorders.” Several of these may be present in elderly patients.
The dose of drugs intended for long-term use in senior patients should generally be kept to the minimum necessary to control clinical signs, as advised in the SPC for methylprednisolone.
In some cases, nutritional supplements may reduce the effective dose of a drug; for example, fish oil containing omega-3 has been shown to reduce dose for carprofen (Fritsch et al, 2010). This is a useful strategy to reduce stress on the liver and kidneys in senior animals.
The following list contains medicines contraindicated or requiring dose adjustment in elderly dogs with hepatic or renal impairment (Allerton, 2023).
Amikacin; renal failure; nephrotoxic; avoid if possible or adjust dose as previously outlined.
Amoxicillin; renal failure; double dosing interval or halve dose.
Amphotericin B; renal failure; nephrotoxic; avoid if possible or adjust dose as previously outlined.
Ampicillin; renal failure; double dosing interval or halve dose.
NSAIDs; renal failure (avoid if possible or adjust dose as previously outlined); or in cases of hepatic insufficiency (avoid if possible or double dosing interval or halve dose); nephrotoxic.
Propanolol; hepatic insufficiency; avoid if possible, or double dosing interval or halve dose.
Theophylline; hepatic insufficiency; avoid if possible, or double dosing interval or halve dose.
Tobramycin; renal failure; nephrotoxic; avoid if possible or adjust dose as previously outlined.
Trimethoprim/sulphonamide; renal failure; nephrotoxic; avoid if possible or increase dosing interval ×2 up to ×4 depending on CCr.
Vincristine; hepatic insufficiency; avoid if possible, or double dosing interval or halve dose.
This is not a comprehensive review of all medicines that may be a problem in senior dogs with renal or kidney impairment, so always review the product datasheet at the VMD before administering medicines and screen the patient for potential problems (www.vmd.defra.gov.uk/productinformationdatabase).
Image: Alex Renko / Adobe Stock
When to screen before administering a drug to an elderly patient
All elderly patients
For cats and dogs in the last third of expected lifespan, it should be considered likely that subclinical age-related diseases will be present, in addition to any clinical signs, so a geriatric screen is advisable.
This becomes even more essential when a patient is in its last quartile of life expectancy. The screen includes a full history and physical examination and diagnostic tests as deemed necessary. It is important to rule in or out commonly seen diseases, such as those previously listed.
Body composition extremes, such as emaciation or obesity, will alter how drugs are used and affect safety and efficacy. Reduced liver or renal function and impaired blood transport mechanisms will alter safety and drug pharmacokinetics and pharmacodynamics. Drug metabolism is altered by changes in:
Transportation – blood/albumin.
Metabolism – liver/other tissues.
Excretion – kidney/liver.
Distribution – water/lipid.
Perioperative period
Many geriatric patients need to undergo surgery. In humans, low serum albumin and inadequate protein-calorie intake increases the risk of postoperative wound infection (Alfargieny et al, 2001; Haydock and Hill, 1986).
In a Cochrane systematic review, pre-surgical immune moderating nutritional supplements were shown to reduce postoperative complication rates, and early feeding postoperatively is also known to be important.
In elderly patients requiring surgical intervention, it is important to:
Evaluate the patient for pre-existing malnutrition.
Treat malnutrition to optimise surgical readiness.
Minimise hyporexia.
Prevent postoperative malnutrition.
Support anabolism for recovery.
Major surgery in elderly patients induces surgical stress, resulting in hyperglycaemia and whole-body protein catabolism causing wasting of lean tissue, including lean muscle mass mobilisation. This releases amino acids into circulation for preferential uptake by the liver to allow the synthesis of acute phase reactants. It also stimulates production of glucose from non-carbohydrate sources via gluconeogenesis.
General anaesthetic agents are lipid soluble (they need to enter the brain to exert their effects) and they may accumulate in adipose tissues and delay recovery.
For opioids – especially if administered intramuscularly – it may be preferable to dose according to the patient’s actual weight, so that, after redistribution into fat, an effective plasma/effect site concentration is achieved and maintained. During prolonged administration of inhalation agents, which may easily occur in obese patients, the blood solubility of the agents becomes less important than their fat solubility for influencing recovery from anaesthesia.
The potential for prolonged recoveries is greatest with halothane, but also potentially a nuisance with sevoflurane and even isoflurane, although isoflurane tends to be the favourite choice. Increased circulating free fatty acids, triglycerides and cholesterol compete with acidic anaesthetic agents for protein-binding with albumin, increasing free/active drug concentrations.
In contrast, the increased alpha-1 acid glycoprotein concentration found in obese states can increase the binding of basic drugs (ketamine, opioids, local anaesthetics), reducing their free/active concentrations.
When to monitor elderly patients on long-term medication
All patients on long-term medications should be monitored regularly for signs of disease progression or changes in drug safety or efficacy and, if necessary, drug dosage or frequency may need to be modified, and in some cases drug choice changed.
In some cases, the drug SPC will advise monitoring, so datasheets should be checked regularly; for example, the SPC for pimobendan states: “The blood glucose should be tested regularly during treatment in dogs with existing diabetes mellitus”, and: “Monitoring of cardiac function and morphology is recommended in animals treated with pimobendan”.
In the SPC of meloxicam for cats, it states: “Chronic musculoskeletal disorders: response to long-term therapy should be monitored at regular intervals by a veterinary surgeon”.
Specific drugs in common use
It is useful to consider some of the key issues specified in drug SPCs .
Diuretics
Widely used in older dogs with cardiac failure, diuretics increase the risk of developing hypokalaemia, so monitor their effects.
The efficacy of furosemide is reduced in elderly patients due to reduced secretion of the drug at site of action (renal tubules).
Furosemide has decreased renal elimination in elderly patients, and relative overdosing can lead to dehydration, azotaemia, hyponatraemia and hypotension.
Diuretics are contraindicated in elderly patients with diabetes, as they can cause hyperglycaemia.
Hypoglycaemics
Hypoglycaemics may cause a decreased clearance rate of insulin and peripheral insulin resistance; for example, secondary to obesity.
NSAIDs
Most NSAIDs are eliminated via the liver and they have serious potential adverse effects, including gastrointestinal haemorrhage and acute kidney injury, leading to renal failure.
Toxic effects of NSAIDs are seen mainly when starting on drugs or when increasing the dose. Dietary interventions have been shown to reduce the dose of NSAID required in the management of osteoarthritis and this is to be recommended. NSAIDs are contraindicated in renal or hepatic disease, so check the product SPC before use, and if it decided to continue to use the drug, make sure it is with fully informed owner consent.
The following list contains selected drugs in common use in elderly patients and SPC information that needs to be considered during use.
Furosemide: contraindicated in acute glomerular nephritis, renal failure with anuria, electrolyte deficiency or digitalis toxicity. Do not use with aminoglycoside antibiotics. The amount of drinking water should be restricted during treatment. Only during prolonged treatment is it necessary to monitor potassium balance, and potassium supplementation may be necessary.
Benazepril: can be given with digoxin, diuretics and anti-arrhythmic drugs. Combined with an NSAID, it can lead to reduced anti-hypertensive efficacy or impaired renal function. Transient hypotension may occur – especially if used in combination with other anti-hypertensive agents such as diuretics, calcium channel blockers, beta blockers, anaesthetics or sedatives. Plasma concentration of potassium should be monitored if using potassium-sparing drugs such as spironolactone. It is recommended to monitor plasma urea and creatinine concentrations (dogs and cats) and erythrocyte counts (cats).
Hypoglycaemics: sulfonylureas can cause hypoglycaemia.
If renal impairment is present, select those eliminated by the liver, such as glipizide or tolbutamide.
Meloxicam: do not use in animals with gastrointestinal disorders or with impaired hepatic, cardiac or renal function or haemorrhagic disorders. Avoid use in dehydrated, hypovolaemic or hypotensive animals. If used with other NSAIDs, diuretics, anticoagulants or aminoglycoside antibiotics, it may lead to toxic effects. It must not be used with other NSAIDs or corticosteroids, or other potentially nephrotoxic drugs, in animals at anaesthetic risk, such as the elderly.
Carprofen: do not use in animals with gastrointestinal disorders or with impaired hepatic, cardiac or renal function or haemorrhagic disorders. Avoid use in dehydrated, hypovolaemic or hypotensive animals. It must not be used with other NSAIDs. Concurrent use with other potentially nephrotoxic drugs should be avoided. According to the SPC: “Use in dogs less than six weeks of age, or in aged dogs, may involve additional risk. If such a use cannot be avoided, such dogs may require a reduced dosage and careful clinical management.” It can cause inhibition of phagocytosis, so use antibiotics if bacterial infection present.
ACP: hypotensive. Care should be taken in hypovolaemic animals. The author has witnessed the death of an elderly dog given a very small intravenous dose of ACP as a premedication. Following administration, the amount of anaesthetic agent necessary to induce anaesthesia is considerably reduced – approximately one-third of normal dose. ACP potentiates barbiturate anaesthesia. Minimum dose should be used in large breeds.
Oclacitinib: do not use in dogs with evidence of immunosuppression, such as hyperadrenocorticism, or with evidence of progressive malignant neoplasia, as the active substance has not been evaluated in these cases. Dogs receiving the veterinary medicinal product should, therefore, be monitored for the development of infections and neoplasia. Periodic monitoring with complete blood counts and serum biochemistry is recommended when dogs are on long-term treatment. Side effects include: pyoderma, skin lump, papilloma (very common); nausea, vomiting, diarrhoea, anorexia (common; 1-10 per 100); histiocytoma, fungal skin infection, pododermatitis, otitis, lymphadenopathy, cystitis, aggression. The major clearance route is metabolism, with minor contributions from renal and biliary elimination.
Bedinvetmab: this veterinary medicinal product may induce transient or persistent anti-drug antibodies. Caution should be used when treating patients with the following pre-existing conditions: immune-mediated haemolytic anaemia, immune-mediated polyarthritis, immune-mediated thrombocytopenia. Caution should be used when treating patients with pre-existing seizure disorders.
Prednisolone: generally contraindicated in patients with renal disease or diabetes mellitus, and where corneal ulceration is present. Some corticosteroids cause sodium and water retention and hypokalaemia. Some cause calcinosis cutis. Corticosteroids depress the immune system, delay wound healing and exacerbate existing infections. Gastrointestinal ulceration may occur, exacerbated by concurrent use of NSAIDs. Steroids cause enlargement of the liver and increased serum hepatic enzymes. As per the BSAVA Formulary, they may cause proteinuria, glomerular changes (dogs), hyperglycaemia and decreased thyroxine.
Polytherapy
Concurrent drug administration is common in elderly patients because of concurrent diseases, but polytherapy is risky, and in some cases the SPC of one drug will advise against such practices; for example, for meloxicam use in cats, the SPC states: “Other NSAIDs, diuretics, anticoagulants, aminoglycoside antibiotics and substances with high protein binding may compete for binding and thus lead to toxic effects. The veterinary medicinal product must not be administered in conjunction with other NSAIDs or glucocorticosteroids. Concurrent administration of potential nephrotoxic drugs should be avoided”.
Summary for use of drugs in elderly patients
Always review SPC (datasheet) recommendations and consider the safest drug option for the individual.
In elderly patients, start at lower than recommended doses.
Give the minimum dose needed to achieve clinical objectives.
Pre-screen before administering drugs with low therapeutic index and serious side effects.
Monitor patients regularly.
Avoid unnecessary polytherapy.
Consider drug-drug and drug-disease interactions.
Use of some of the drugs in this article is under the veterinary medicine cascade.
This article appeared in Vet Times (17 March 2026), Volume 56, Issue 11, Pages 10-14
Mike Davies qualified from the RVC, has RCVS postgraduate certificates in veterinary radiology and small animal orthopaedics, and holds a fellowship by examination in clinical nutrition in cats and dogs. He is an RCVS specialist in veterinary nutrition (small animal clinical nutrition). Mike has worked in academia and private practice, and for several pet food manufacturers and pharmaceutical companies. He speaks internationally on clinical nutrition and geriatrics, and founded the original City and Guilds certificate in small animal nutrition, and the BVNA certificates in small animal and exotic nutrition. He runs Provet’s certificate course in clinical nutrition.
Alfargieny R, Bodalal Z, Bendardaf R et al (2015). Nutritional status as a predictive marker for surgical site infection in total joint arthroplasty, Avicenna J Med5(4): 117-122.
Allerton F (2023). BSAVA Small Animal Formulary Part 1: Canine and Feline (11th edn), BSAVA, Gloucester: 420.
Davies M (1996). Canine and Feline Geriatrics (Library of Veterinary Practice), Blackwell Science, Oxford.
Fritsch DA, Allen TA, Dodd CE et al (2010). A multicenter study of the effect of dietary supplementation with fish oil omega-3 fatty acids on carprofen dosage in dogs with osteoarthritis, J Am Vet Med Assoc236(5): 535-539.
Haydock DA and Hill GL (1986). Impaired wound healing in surgical patients with varying degrees of malnutrition, JPEN J Parenter Enteral Nutr 10(6): 550-554.
Herbert G, Perry R, Andersen HK et al (2019). Early enteral nutrition within 24 hours of lower gastrointestinal surgery versus later commencement for length of hospital stay and postoperative complications, Cochrane Database Syst Rev10(7): CD004080.
Morgan DJ and Bray KM (1994). Lean body mass as a predictor of drug dosage. Implications for drug therapy, Clin Pharmacokinet26(4): 292-307.